Downloaded 10 times
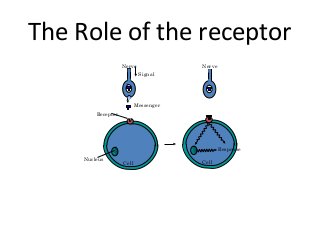

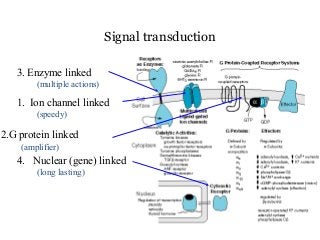
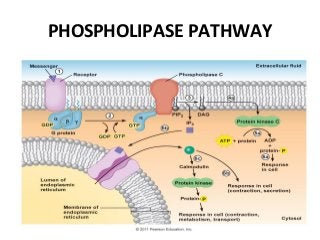
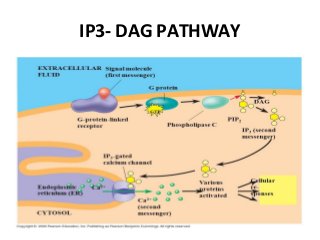
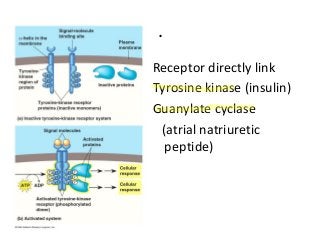
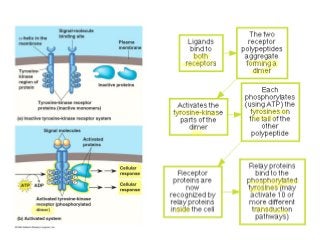
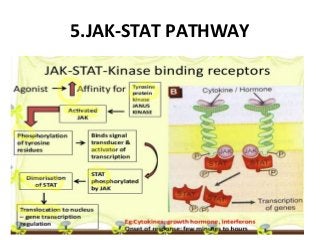
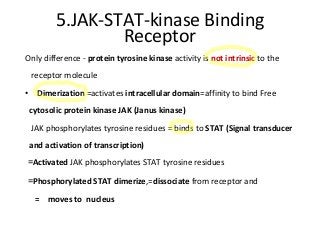
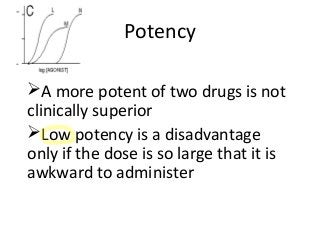
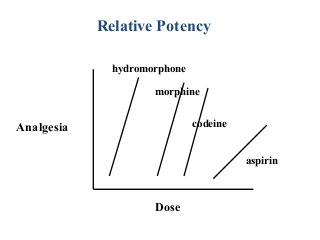


This document provides an overview of pharmacodynamics, which is the study of how drugs act on the body. It discusses several key concepts: 1. Most drugs act by binding to receptors on or within cells. This can open or close ion channels, activate second messengers, or physically inhibit cellular functions. 2. Drugs can bind to different types of receptors like G-protein coupled receptors or tyrosine kinase receptors, activating various signal transduction pathways. 3. Affinity refers to how strongly a drug binds to its receptor, while efficacy refers to its ability to produce an effect after binding. Potency is the amount needed to produce a half-maximal effect. 4. Therapeutic











































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











