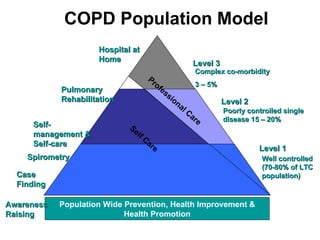
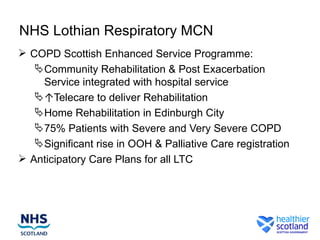
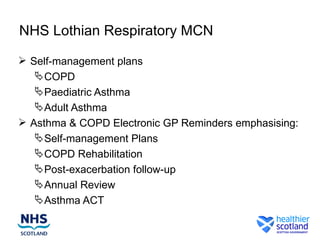
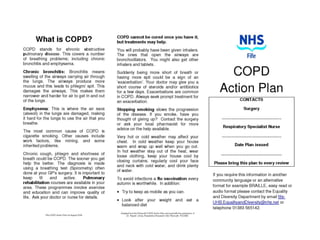
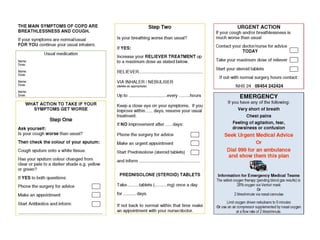
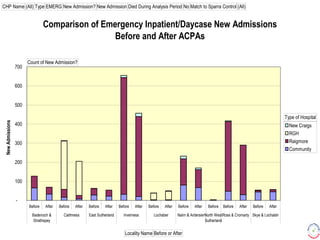
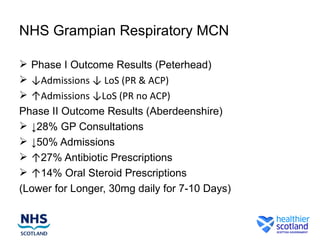
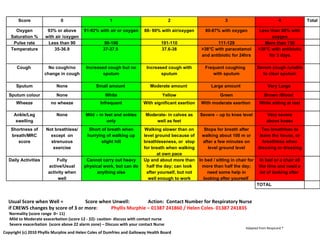
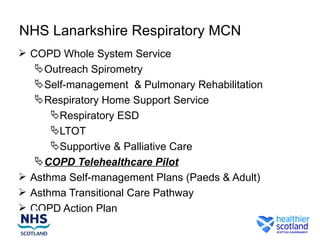
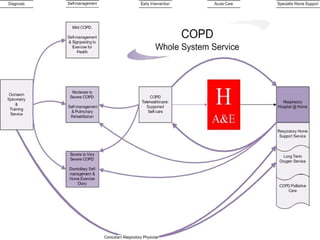
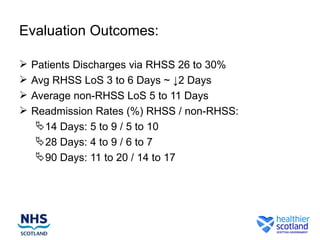
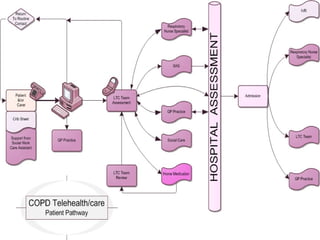
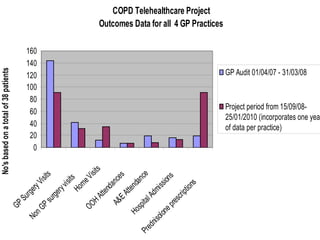
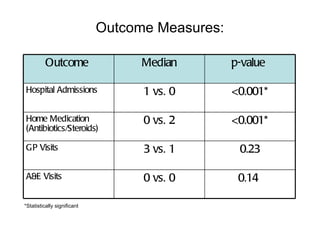
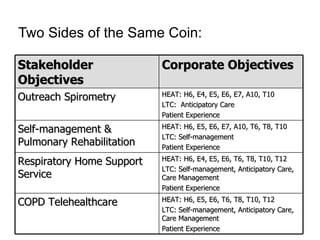
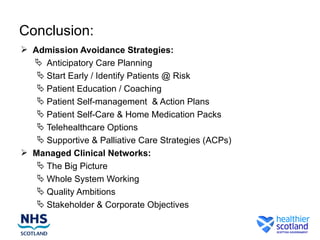
The document describes respiratory care strategies from several NHS boards in Scotland. It discusses initiatives like anticipatory care plans, pulmonary rehabilitation programs, self-management plans for COPD and asthma, telehealth/telemonitoring pilots, and community respiratory warning systems. Several boards reported reductions in hospital admissions, length of stay, and bed occupancy from these anticipatory care strategies.