



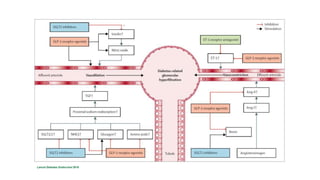



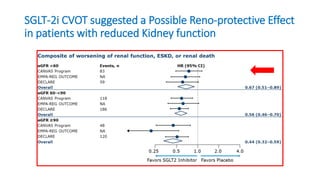
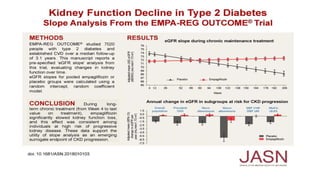





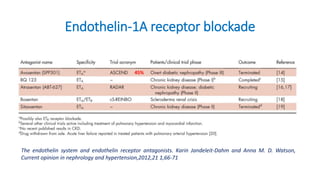

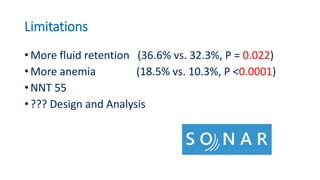
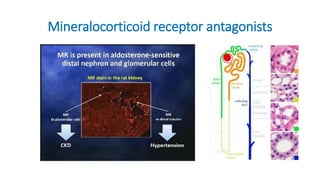
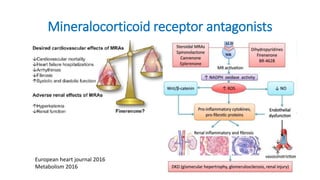

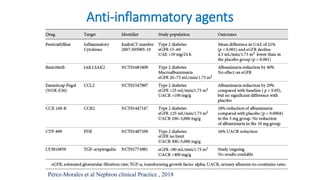
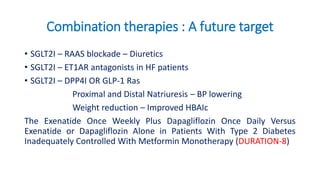
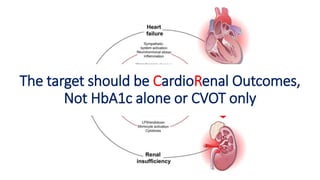


Diabetic kidney disease remains a major global health problem. Recent research has provided insights into the pathophysiology and has identified new diagnostic and therapeutic approaches. Several large clinical trials have shown that sodium-glucose cotransporter-2 inhibitors, glucagon-like peptide-1 receptor agonists, mineralocorticoid receptor antagonists, and endothelin receptor antagonists can reduce kidney disease progression and cardiovascular events in patients with diabetes and kidney disease. Ongoing trials are further evaluating combination therapies and the benefits of these agents in non-diabetic kidney disease and heart failure.











































































