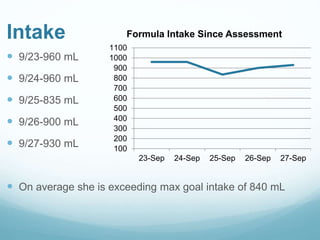
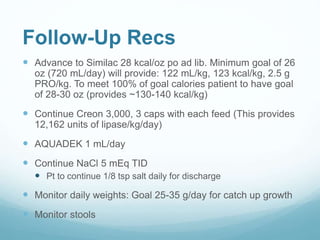
This document provides information on cystic fibrosis including signs and symptoms, nutrition implications, and treatment. It then presents a case study on a 9.8 month old female patient with CF who was admitted for metabolic insufficiencies. Initial assessment found the patient was underweight. Recommendations included increasing formula intake and supplements. Follow up found weight gain and increased intake meeting goals. Further advancement of formula was recommended.









![Cystic fibrosis presentation [autosaved] final](https://cdn.slidesharecdn.com/ss_thumbnails/cysticfibrosispresentationautosavedfinal-161019122332-thumbnail.jpg?width=640&height=640&fit=bounds)

























































