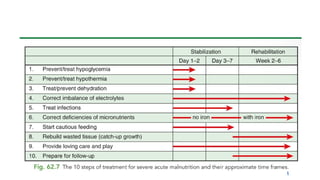
SAM MANAGEMENT
TEN STEPS-
1.HYPOGLYCEMIA
2.HYPOTHERMIA
3.DEHYDRATION
4.ELECTROLYTE CORRECTION
5.INFECTIONS.
6MICRONUTRIENTS
7. INITIATE FEEDING
8.CATCH UP GROWTH
9.SENSORY STIMULATION
10.FOLLOWUP
4.
EMERGENCY TREATMENT-
SHOCK
• Lethargicor unconscious
• Cold hands
Plus either:
• CRT >3 sec or
• Weak pulse.
Hypoglycemia and hypothermia
and infection often coexist .
5.
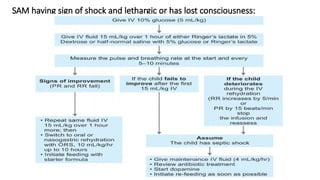
SAM having signof shock and lethargic or has lost consciousness:
6.
Asymptomatic
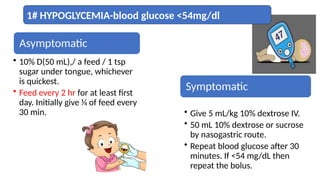
• 10% D(50mL),/ a feed / 1 tsp
sugar under tongue, whichever
is quickest.
• Feed every 2 hr for at least first
day. Initially give 1⁄4 of feed every
30 min.
Symptomatic
• Give 5 mL/kg 10% dextrose IV.
• 50 mL 10% dextrose or sucrose
by nasogastric route.
• Repeat blood glucose after 30
minutes. If <54 mg/dL then
repeat the bolus.
1# HYPOGLYCEMIA-blood glucose <54mg/dl
7.
• Feed every3 hr day and night
(2 hr if ill).
• Feed on time.
• Keep warm.
• Treat infections
Prevention-
Avoid long
gaps without
food and
minimize
need for
glucose.
8.
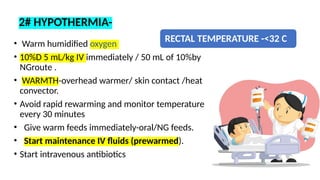
RECTAL TEMPERATURE -<32C
• Warm humidified oxygen
• 10%D 5 mL/kg IV immediately / 50 mL of 10%by
NGroute .
• WARMTH-overhead warmer/ skin contact /heat
convector.
• Avoid rapid rewarming and monitor temperature
every 30 minutes
• Give warm feeds immediately-oral/NG feeds.
• Start maintenance IV fluids (prewarmed).
• Start intravenous antibiotics
2# HYPOTHERMIA-
9.
HYPOTHERMIA-
Axillary temperature <35°C
orrectal temperature <35.5°C
Lethargy and poor feeding
• Cover the head by cap and
limbs by socks and mitten
• Kangaroo mother care
10.
Preventio
n
• Maintain
room
temperatur
e of25°C
• Feed
immediat
ely and
then
regular
interval
• Cover the
child
including
head,
soles, and
palm
• Stop
draughts
in the
room
•
Promptly
change
wet
clothes or
bedding
11.
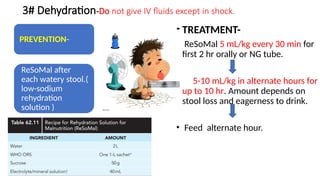
3# Dehydration-Do notgive IV fluids except in shock.
PREVENTION-
ReSoMal after
each watery stool.(
low-sodium
rehydration
solution )
• TREATMENT-
• ReSoMal 5 mL/kg every 30 min for
first 2 hr orally or NG tube.
• 5-10 mL/kg in alternate hours for
up to 10 hr. Amount depends on
stool loss and eagerness to drink.
• Feed alternate hour.
13.
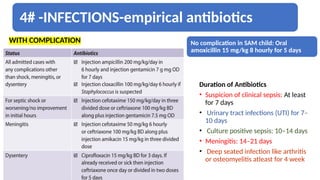
4# -INFECTIONS-empirical antibiotics
WITHCOMPLICATION No complication in SAM child: Oral
amoxicillin 15 mg/kg 8 hourly for 5 days
Duration of Antibiotics
• Suspicion of clinical sepsis: At least
for 7 days
• Urinary tract infections (UTI) for 7–
10 days
• Culture positive sepsis: 10–14 days
• Meningitis: 14–21 days
• Deep seated infection like arthritis
or osteomyelitis atleast for 4 week
5# Correct electrolyteimbalance—deficit of potassium and
magnesium, excess sodium
• Potassium chloride: 3–4 mEq/kg/d for 14 days.
• Magnesium sulfate:
• 0.3 mL/kg of maximum 2 mL intramuscular followed by
0.3 mL/kg orally for 13 days .
• Food without added salt in order to avoid sodium
• Do not treat edema with diuretics
16.
• Very severeanemia
• Hb 4-6g/dL and respiratory distress.
• Whole blood 10 mL/kg –IV over 3-4
hr.
• signs of heart failure- 5-7 mL/kg
packed cells.
• Furosemide 1 mg/kg IV at the start
of the transfusion.
• Emergency eye care/Corneal
ulceration
• vitamin A immediately (age <6
mon: 50,000 IU; 6-12 mon:
100,000 IU; >12 mon: 200,000
IU)
• Instill 1 drop atropine (1%) into
affected eye to relax the eye and
prevent the lens from pushing
out.
17.
Micronutrient deficiencies-
• Onadmission and given for 2 weeks.
• Iron - 3 mg/kg is started after 7 days of admission.
• vitamin A on day 1 (<6 mon 50,000 units; 6-12 mon 100,000 units; >12
mon 200,000 units).
• Eye signs of vitamin A deficiency or has had recent measles. Repeat this
dose on days 2 and 14.
18.
• Multivitamin supplement(should contain vitamin A, C, D, E, and B12 and
not just vitamin B complex): Twice recommended daily allowance.
• Folic acid: 5 mg stat then 1 mg for 13 days.
• Zinc: 2 mg/kg for 14 days.
• Copper: 0.3 mg/kg.
• Iron: 3 mg/kg/day to be started after 7 days of patient admission
• Cautious feeding .
Zinc
I
r
o
n
19.
Stabilisation phase:
• Aim-achieve weight for height.
• Calories - 150–200 kcal/kg/day. 4 g protein and 100–150 mL/kg of
water per day.
• Calorie requirements - actual weight.
• Initially liquid diet started-divided into 6–8 feeds/day including a late
night and an early morning feed to prevent hypoglycaemia in night.
• Tube feeds -severe anorexia and apathy.
• Vitamins and micronutrients .
• Deworming .
• Family pot feeding.
20.
Starter Diet:
• 8-12small feeds -130mL/kg/day, F75- 75kcal/100ML, 1-1.5g
protein/kg/day.
• Edema-100 mL/kg/day.
• Keep a 24-hr intake chart. Measure feeds carefully. Record leftovers.
• If child has poor appetite, encourage to finish the feed.
• If unfinished, reoffer later.
NG tube if eating ≤80% .
Encourage continued breastfeeding /F75.
• Daily wg monitoring.
21.
Rehabilitation phase
• Aim-weight for age/food supplementation along with
rehabilitation.
• To prevent -back to PEM again by maintaining adequate
nutrition/ periodic growth monitoring/
immunization/routine medical care.
• Health education.
• Reduced or minimal edema and return of appetite.
• F75 F100 ( 100 kcal and 3 g protein per 100 mL),
or ready-to-use therapeutic food RUTF.
22.
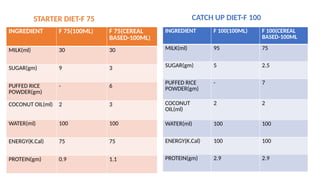
• If F-75and F-100 are not available.
• Calculate the amount of starter feed (prepared with cow’s milk, sugar,
rice powder, and vegetable oil to provide approximately 75 kcal and
0.9 g protein per 100 mL) .
• Catch-up diet (to provide approximately 100 kcal and 2.9 g protein
per 100 mL) to be offered .
• Based on daily weight measured.
9#-Provide sensory stimulationand emotional support.-
reduces the risk of permanent mental retardation and emotional impairment.
• A cheerful ,stimulant environment.
• Age appropriate structured play therapy for atleast 15-30min.
• Tender loving care.
26.
Discharge from NutritionRehabilitation Centre
• Edema- resolved
• weight gain >15% and satisfactory weight gain for 3 consecutive days
(>5 gm/kg/day).
• Child is eating an adequate amount of nutritious food that the
mother can prepare at home.
• All infections and other medical complications treated.
• Micronutrients.
• Immunization is updated.
27.
• Failure criteriaof SAM
management:
• Day 4.
• Failure to gain appetite.
• Failure to start to lose edema.
• Day 10
• Edema still present
• Failure to gain at least 5 g/day
for 3 successive days.
• After feeding freely on catch-up
diet.
• Look for the cause of failure:
• Insufficient food given.
• Vitamin or mineral deficiency.
• unrecognized infections.
28.
• Mother/caregiver:
Toprepare appropriate foods and to feed the child.
Give prescribed medications, vitamins, folic acid and iron at home.
To make appropriate toys and play with the child.
To give home treatment for diarrhoea, fever and acute respiratory
infections .
To recognize the signs for which medical assistance needed.
Follow-up plan is discussed and understood.
community based program is well functioning, child can be
transferred from facility based care to community based care for
achieving target weight gain of 15 %.
30.
Outcome and prognosis
•Long term effects-stature,developmental,cognitive function.
• 1st
6month-stunted despite treatment-25-60%
• Early diagnosis and intervention –needed to prevent long term
effects.
32.
Take home message!
•Be Slow and steady ,No aggressive treatment.
• No diuretics for edema
• No iv fluids for dehydration(except in shock).
• No high protein diet in early phase of treatment.
• Low sodium diet .
• No iron therapy in stabilisation phase.
33.
References
-Nelson text bookof pediatrics
22nd
edition.
-Guideline for IP treatment of
SAM-WHO.
-ICMR ,NIN guideline.
-STG-IAP.