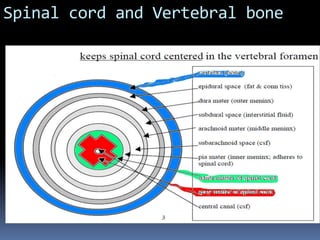
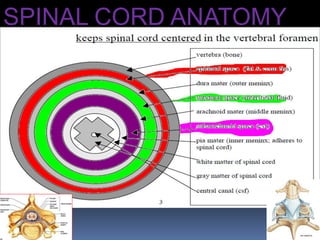
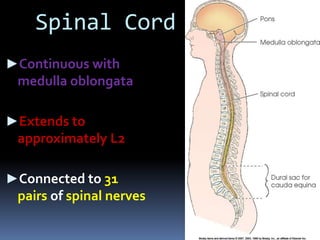
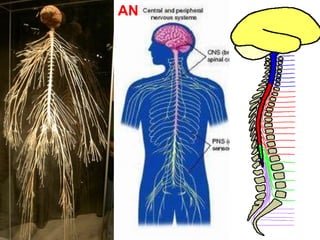
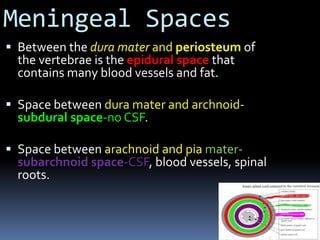
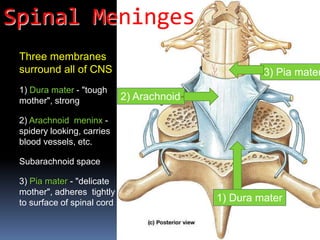
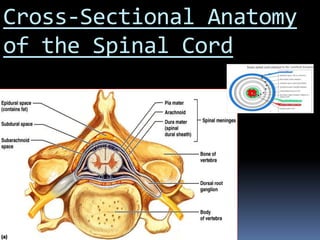
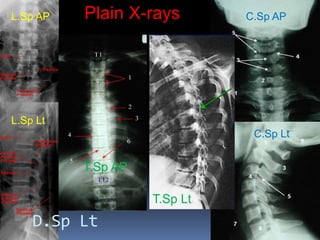
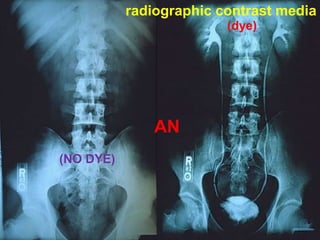
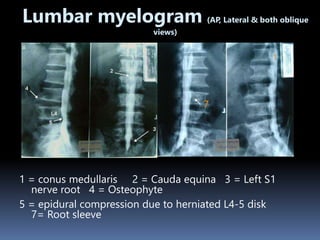
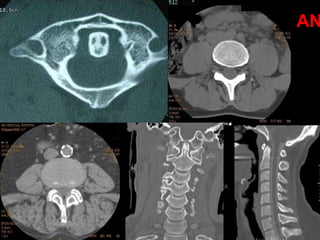
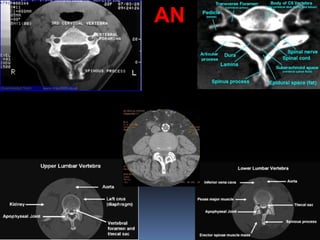
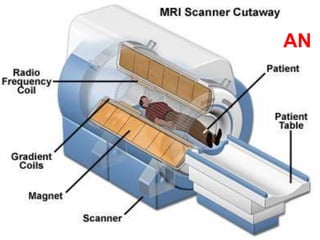
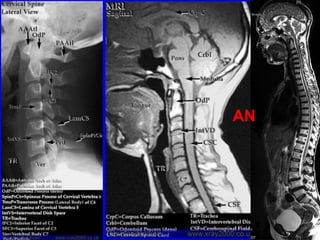
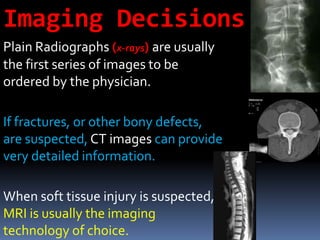
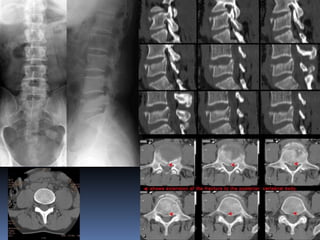
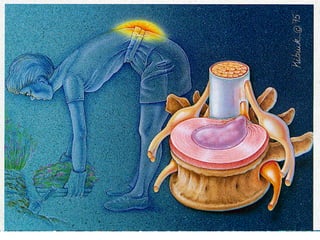
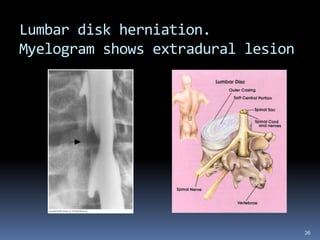
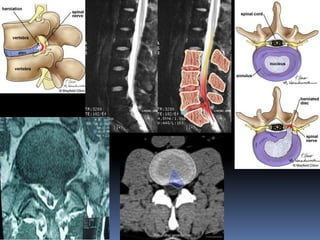
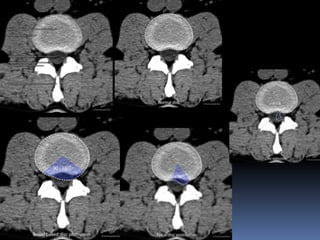
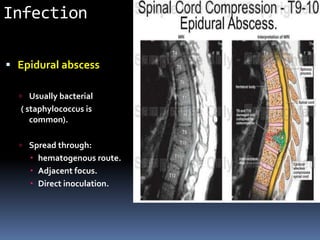
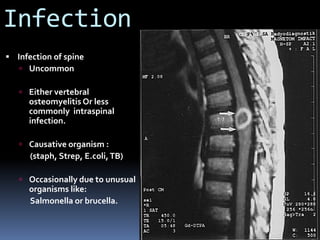
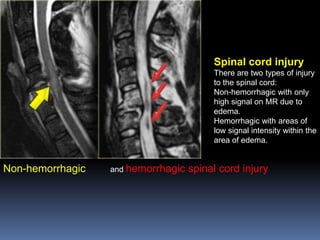
This document provides an overview of radiology of the spinal cord. It begins with an introduction and outlines the topics to be covered, including anatomy of the spinal cord and vertebral column, various radiological investigations such as plain X-rays, myelograms, CT, CT myelograms, and MRI. It then describes the anatomy of the spinal cord and vertebral bones, different radiological methods, and provides examples of the radiological presentation of some spinal cord diseases such as disk herniation, infection, fracture-dislocation, and spinal cord injury.