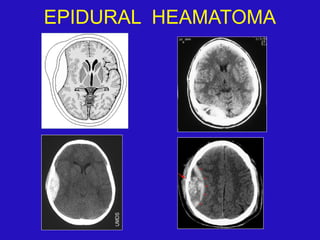
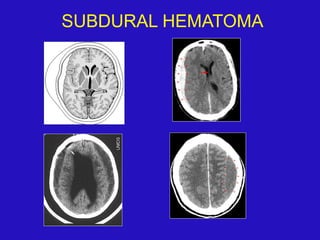
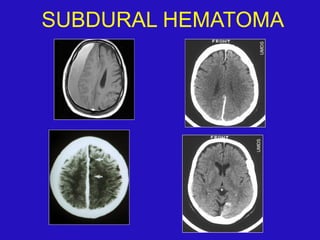
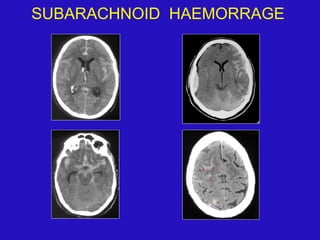
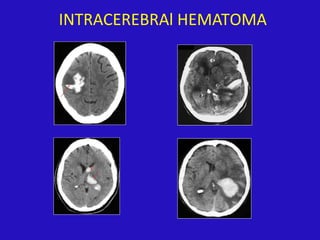
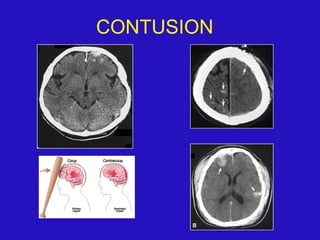
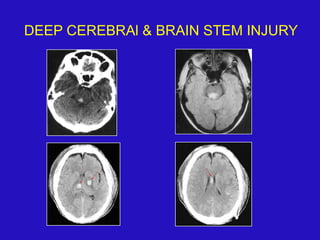
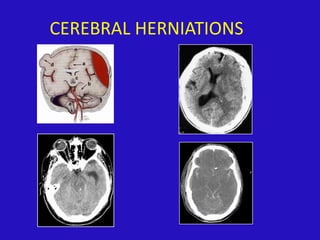
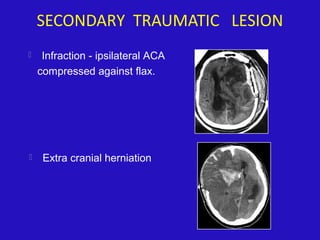
CT is the most important imaging modality for evaluating head trauma. It can detect fractures, extra-axial hemorrhages such as epidural hematomas and subdural hematomas, subarachnoid hemorrhage, intraventricular hemorrhage, and intracerebral hemorrhages. Common primary traumatic brain injuries seen on CT include contusions, diffuse axonal injury characterized by small hemorrhages, and deep cerebral and brainstem injuries. MRI can provide additional details, especially in the subacute and chronic stages.