Downloaded 62 times
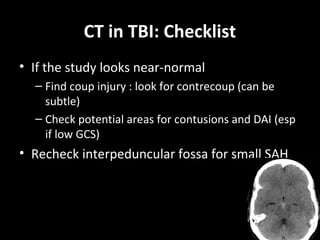
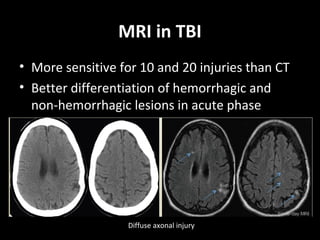


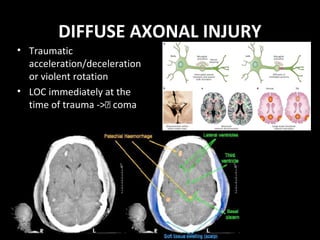

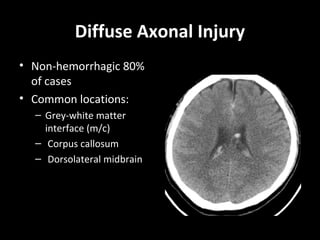

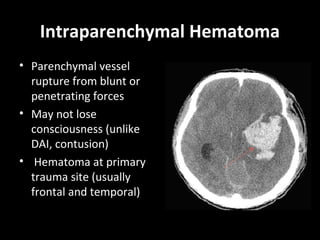
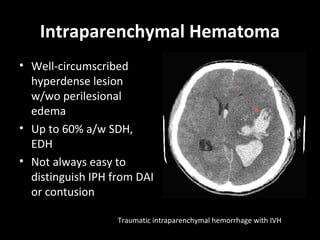
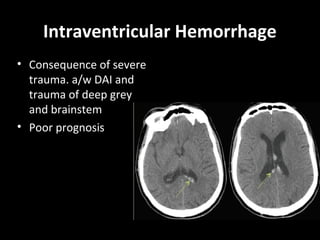

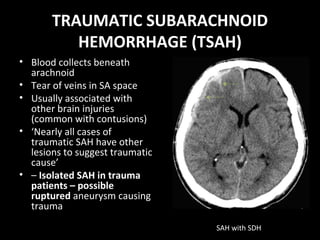
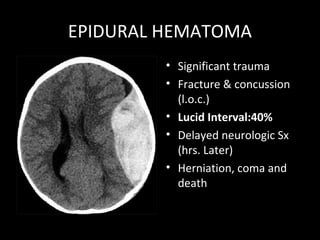
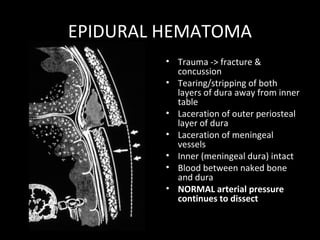
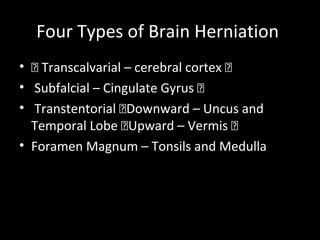

1. The document reviews key imaging findings and goals in traumatic brain injury (TBI) evaluation including recognizing life-threatening injuries like epidural hematoma, diffuse axonal injury, and herniations. 2. CT is recommended for rapid diagnosis in trauma but MRI is more sensitive for injuries like diffuse axonal injury. Imaging helps assess prognosis and guide management. 3. Specific lesions discussed include intraparenchymal hemorrhage, subdural hematoma, subarachnoid hemorrhage, skull fractures, cerebral edema, and traumatic vascular injuries. Characteristic appearances on CT and clinical implications are reviewed.


































































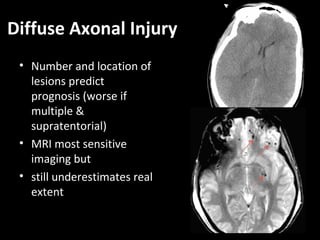
![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











