



![A study testing the ability of these proposed criteria to
differentiate between CRPS and non-CRPS neuropathic
pain groups suggested that a modification of the Orlando
IASP/CRPS diagnostic criteria could improve overall diag-
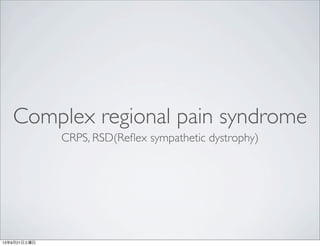
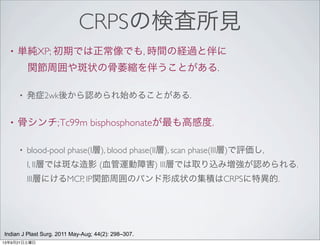
nostic accuracy [21–23]. Results showed that employing a
decision rule requiring two of four sign categories and four
of four symptom categories for a positive diagnosis
resulted in a sensitivity of 0.70 and a specificity of 0.94. Of
all those tested, this decision rule resulted in the highest
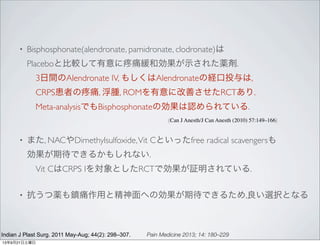
Table 5 Clinical diagnostic criteria for complex
regional pain syndrome
1) Continuing pain, which is disproportionate to any
inciting event
2) Must report at least one symptom in three of the four
following categories
Sensory: Reports of hyperalgesia and/or allodynia
Vasomotor: Reports of temperature asymmetry and/or
skin color changes and/or skin color asymmetry
Sudomotor/Edema: Reports of edema and/or sweating
changes and/or sweating asymmetry
Motor/Trophic: Reports of decreased range of motion
and/or motor dysfunction (weakness, tremor, dystonia)
and/or trophic changes (hair, nail, skin)
3) Must display at least one sign* at time of evaluation in
two or more of the following categories
Sensory: Evidence of hyperalgesia (to pinprick) and/or
allodynia (to light touch and/or deep somatic pressure
and/or joint movement)
Vasomotor: Evidence of temperature asymmetry
and/or skin color changes and/or asymmetry
Sudomotor/Edema: Evidence of edema and/or
sweating changes and/or sweating asymmetry
Motor/Trophic: Evidence of decreased range of motion
and/or motor dysfunction (weakness, tremor, dystonia)
and/or trophic changes (hair, nail, skin)
4) There is no other diagnosis that better explains the
signs and symptoms
* A sign is counted only if it is observed at time of diagnosis.
Pain Medicine 2013; 14: 180–229
症状が4/4,
所見が2/4を満たす場合は,
感度70%, 特異度94%
samples (minimizing false-positives) vs identification of the
highest number of CRPS patients possible (minimizing
false-negatives). The Budapest consensus panel therefore
implemented a different set of decision rules for proposed
clinical criteria (see Table 5), requiring two of four sign
categories and three of four symptom categories to be
positive [27]. This ostensibly minor adjustment (merely
requiring three rather than four symptoms) resulted in a
sensitivity of 0.85 and a specificity of 0.69, which repre-
sented a good compromise in identifying as many patients
as possible at an acceptably accurate rate in the clinical
context (see Table 5; for a summary of the sensitivity and
specificity of the two criteria, see Table 7). Recently, the
Committee for Classification of Chronic Pain of the IASP
has accepted and codified the “Budapest” criteria for
clinical and research diagnosis (Table 3). In response to
the consensus group’s concern with the approximately
15% of patients previously diagnosed with CRPS, a third
diagnostic subtype called CRPS-not otherwise specified
CRPS Stages? CRPS Subtypes?
Is CRPS a uniform phenomenon across individuals, or are
there distinct subtypes and/or stages of the syndrome?
This issue addressing whether or not patient presenta-
tions (i.e., the overall pattern of CRPS signs and symp-
toms) tend to be similar across individuals requires
validation. Historically, three progressive stages of CRPS
have been cited as important in identifying and treating the
syndrome (e.g., [4,28,29]), but the existence of such
sequential stages is a clinical lore, an unsubstantiated
theory based on certain authors’ experience rather than
an outcome of specific scientific study (level 4). This
hypothesized staging can be tested by using cluster
analysis to bracket CRPS patients into three subgroups
delineated according to similarity of signs and symptoms.
If the theorized stages exist, the subsequent statistically
derived patient subgroups should vary considerably with
regard to pain duration (i.e., predictable progress of CRPS
through the three stages should take place); furthermore,
the clinical presentation within the three subgroups should
correspond to the three assumed stages of CRPS (best
described in Bonica [4]).
One hundred and thirteen patients meeting IASP criteria
for CRPS went through standardized history and physical
examinations designed to evaluate CRPS signs and
Motor/Trophic: Evidence of decreased range of motion
and/or motor dysfunction (weakness, tremor, dystonia)
and/or trophic changes (hair, nail, skin)
4) There is no other diagnosis that better explains the
signs and symptoms
* A sign is counted only if observed at time of diagnosis.
Table 7 Summary of sensitivity and specificity of the clinical and research criteria
Criterion Type
Symptom Categories
Required for Diagnosis
Sign Categories
Required for Diagnosis Sensitivity Specificity
Clinical Ն3 Ն2 0.85 0.69
Research =4 Ն2 0.70 0.96
13年9月21日土曜日](https://image.slidesharecdn.com/crps-130921063005-phpapp02/85/Crps-8-320.jpg)


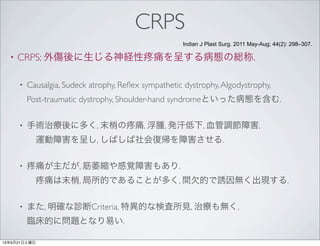
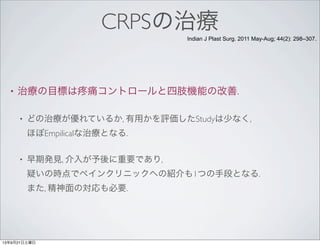
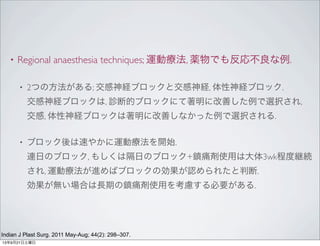
![with a duration of less than 3 months. In our study, TBPS
was also particularly helpful when it was performed in the
first 6 months. Figure 2 shows the TBPS images in a partial
form. Taking all these results together, the role of TBPS in
the diagnosis of CRPS is still uncertain. It is certainly not a
screening tool for diagnosis of CRPS in which clinical find-
ings remain the gold standard. Nevertheless, we believe that
TBPS should be only recommended in the first months of
the disease progression for unclear situations which do not
fully meet the Budapest criteria [29,30]. Based on the pre-
sent knowledge, we have proposed a diagnosis flow chart
(Figure 3) on the application of the Budapest criteria and of
radiology in cases of partial CRPS.
The disease course, reported briefly in the literature, is
described as favourable in the majority of cases (see Table 1),
was modest. Nearly half of our patients (47%) reported im-
provement of at least 30% in pain, which is considered the
smallest clinically significant change that could be detected
[31]. The patients’ perception of global improvement was
more than 50 mm and can be defined as clinically signifi-
cant change (i.e. more than 30 mm) in 80% of patients. This
more global parameter probably reflects patient satisfaction
with the whole interdisciplinary rehabilitation process. Re-
garding return to work, in our series, 50% of patients didn’t
return to work with a follow up of 4 to 9 years. We cannot
explain this long lasting sick leave but none of our patients
had an invalidity pension related to CRPS. The literature is
not very precise, especially concerning return to work, and
to date our study is the first to use detailed insurance data.
Hence, it could happen that old studies may have been
Figure 2 Three-phase bone scintigraphy: early phase (a) and delayed phase (b) Same patient as Figure 1. Staged early and delayed
hyperfixation on 4th
and 5th
fingers suggesting CRPS stage 1.
BMC Neurology 2013, 13:28
13年9月21日土曜日](https://image.slidesharecdn.com/crps-130921063005-phpapp02/85/Crps-13-320.jpg)

![the emerging trend of state-by-state legalization of
medical marijuana improves the feasibility of such a trial.
Botulinum toxin type A used for years to weaken specific
muscles in movement disorders and spasticity works by
available in generic formulation [216]. It may have efficacy
in some local or focal CRPS phenomena such as allodynia
(level 4 evidence) [217]. Capsaicin, the vanilloid compound
in chili peppers, is a highly selective agonist for the tran-
sient receptor potential channel, vanilloid-receptor type 1
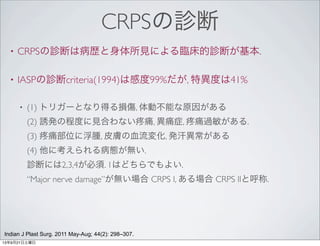
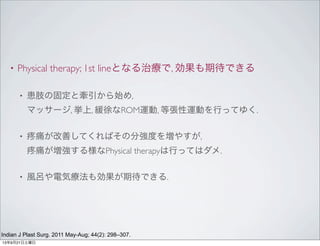
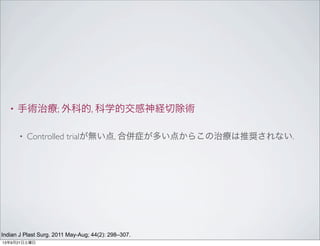
Table 9 Pharmacotherapy guide. The following strategies are suggested for patients who have been
diagnosed with CRPS but who cannot begin or progress in the functional restoration algorithm
Reason for Inability
to Begin or Progress Action
Mild-to-moderate pain Simple analgesics and/or blocks (see interventional therapy section)
Excruciating, intractable pain Opioids and/or blocks or later, more experimental interventions (see interventional
therapy section)
Inflammation/swelling and edema Steroids, systemic or targeted (acutely) or NSAIDs (chronically); immune modulators
Depression, anxiety, insomnia Sedative, analgesic antidepressant/anxiolytics and/or psychotherapy (see
pharmacotherapy section)
Significant allodynia/hyperalgesia Anticonvulsants and/or other sodium channel blockers and/or NMDA receptor
antagonists
Significant osteopenia, immobility
and trophic changes*
Calcitonin or bisphosphonates
Profound vasomotor disturbance Calcium channel blockers, sympatholytics, and/or blocks (see interventional therapy
section)
It is important to remember that these suggestions are overruled by individual patient presentation.
* It is also important to note that certain drugs, such as calcitonin, may be associated with analgesia as well as the more primary
action.
CRPS = complex regional pain syndrome; NMDA = N-methyl-D-aspartate; NSAID = nonsteroidal anti-inflammatory drug.
CRPS Diagnostic and Treatment Guidelines
Pain Medicine 2013; 14: 180–229
13年9月21日土曜日](https://image.slidesharecdn.com/crps-130921063005-phpapp02/85/Crps-21-320.jpg)


Complex regional pain syndrome (CRPS) is characterized by persistent pain that occurs after trauma and is disproportionate to the inciting event. It involves pain, swelling, sweating changes, and motor dysfunction localized to limbs, often impairing social reintegration. CRPS is diagnosed clinically based on symptoms in 3 of 4 categories (sensory, vasomotor, sudomotor/edema, motor/trophic) and signs in 2 categories. While diagnostic criteria lack sensitivity and specificity, the Budapest criteria improved accuracy with 2 symptom and 2 sign categories required. CRPS may involve 3 stages defined by increasing pain, dysfunction and trophic changes, though distinct stages are not validated.




![[DL輪読会]1次近似系MAMLとその理論的背景](https://cdn.slidesharecdn.com/ss_thumbnails/20190412kondo-190412002418-thumbnail.jpg?width=640&height=640&fit=bounds)


































![CRPS ppt sajad final final [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/crpspptsajadautosaved-250921194258-ec8857be-thumbnail.jpg?width=640&height=640&fit=bounds)






![COMPLEX REGIONAL PAIN SYNDROME [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/complexregionalpainsyndromeautosaved-240617174113-5512c3fe-thumbnail.jpg?width=640&height=640&fit=bounds)
















































