

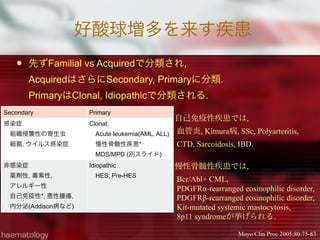
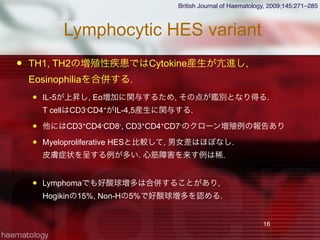
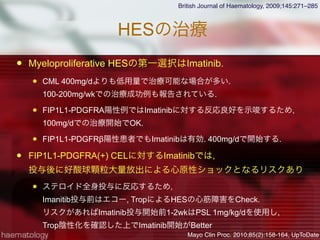
![Myeloproliferative HES variant
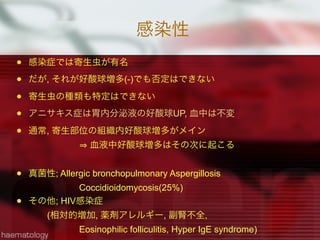
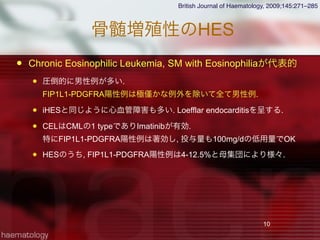
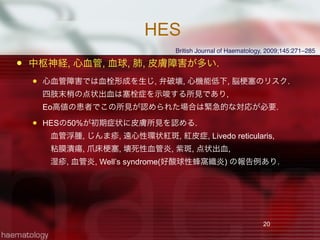
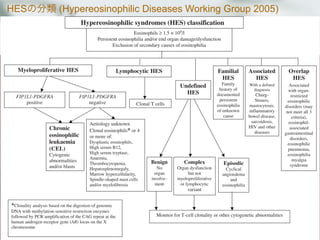
iHESとCELは病態, 経過が似ている.
両者の鑑別にはFIP1L1-PDGFRα [del(4)(a12a12]の検出が重要
Hypereosinophiliaを呈する血液疾患との鑑別
Blood. 2004;103:2879-2891
2次性好酸球増多を除外
FIP1L1-PDGFRαチェック
陽性; FIP1L1-PDGFRα Clonal Eosinophilia
Chronic Eosinophilic Leukemia
Systemic mastocytosis with Eosinophilia
陰性
CEL, Unclassified
T-cell associated HES
HES
異常T cell検出
ClonalなEo増加, 細胞異常
骨髄芽球 5-19%
Clonalな異常無し
異常T cell無し](https://image.slidesharecdn.com/random-130527195759-phpapp02/85/slide-11-320.jpg)
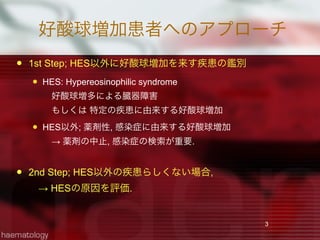
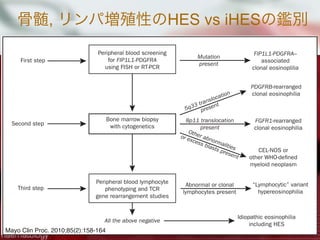
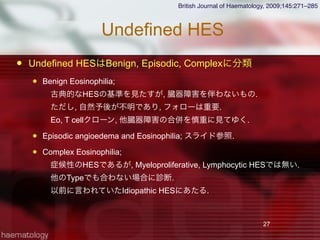
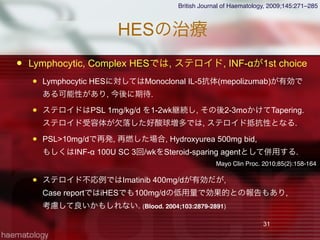
![Systemic
Mastcytosis
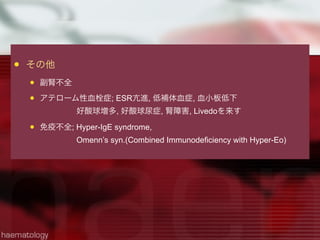
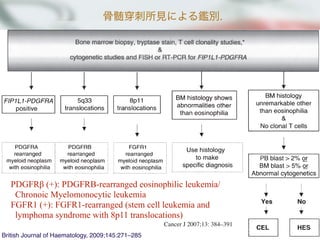
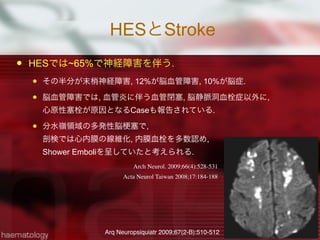
WHOではSMを7つに分類.
WHOのSM診断Criteria
Major 1つ+ Minor 1つ
もしくはMinor 3つで診断.
14
Cancer J 2007;13: 384–391
TABLE 3. “B” Findings: Indication of High Mast Cell Burden
1. Infiltration grade (mast cells) in Ͼ30% in bone marrow on histologic examination and serum total tryptase levels Ͼ200 ng/mL
2. Hypercellular marrow with loss of fat cells, discrete signs of dysmyelopoiesis without substantial cytopenias or WHO criteria for
syndrome or myeloproliferative disorder
3. Organomegaly: palpable hepatomegaly, splenomegaly, or lymphadenopathy (on computed tomography scan or ultrasound) Ͼ2 cm
function
Data from Ref. 65.
TABLE 4. “C” findings: Indication of Impaired Organ Function Attributable to Mast Cell Infiltration66
1. Cytopenia(s): absolute neutrophil count Ͻ1,000/L, or hemoglobin Ͻ10g/dL, or platelets Ͻ100,000/L
2. Hepatomegaly with ascites and impaired liver function
3. Palpable splenomegaly with hypersplenism
4. Malabsorption with hypoalbuminemia and weight loss
5. Skeletal lesions: large-sized osteolysis or severe osteoporosis causing pathologic fractures
6. Life-threatening organopathy in other organ systems that definitively is caused by an infiltration of the tissue by neoplastic mast c
Data from Ref. 66.
TABLE 5. WHO Criteria for Diagnosis of SM*
Major
Multifocal dense infiltrates of mast cells in bone marrow or other extracutaneous organ sections (Ͼ15 mast cells aggregating)
Minor
a. Ն25% mast cells in tissue sections or bone marrow aspirate smear are spindle shaped or have atypical morphology
b. c-kit point mutation at codon 816V
c. Expression of CD2 and/or CD25 by mast cells
d. Baseline serum tryptase persistently Ͼ20 ng/mL (not valid in presence of another non–mast cell clonal disorder)
al residual disease after imatinib therapy can be as-
by quantitative molecular analysis.44
PDGFRB rearrangement was first characterized in the
of a fusion tyrosine kinase encoding regions of
RB and the ets-like gene, ETV6 [ETV6-PDGFRB,
(q33;p13)].46 At present, several other PDGFRB fu-
anscripts are known to exist and are associated with
nt myeloproliferative neoplasm (MPN) phenotypes
ted with eosinophilia.47–55 As has been seen in indi-
with PDGFRA-rearranged MPNs, imatinib therapy
es complete hematologic remission in PDGFRB-rear-
clonal eosinophilia.48,49,51,55–57
FGFR1 translocations are usually associated with a clin-
enotype with features of both an aggressive, eosinophilia-
ted MPN and T cell lymphoblastic lymphoma.58 The
site syndrome is known as either the 8p11 myeloprolif-
syndrome or stem cell leukemia lymphoma syndrome
molecularly characterized by fusion of various 5Ј partner
o the 3Ј part of FGFR1, making it constitutively active.
utation is present in both myeloid and lymphoid lineage
–63 Clinically, 8p11 myeloproliferative syndrome/stem
kemia lymphoma syndrome has an aggressive clinical
with a rapid transformation into acute leukemia. At
, drug therapy is ineffective and allogeneic stem cell
antation should be considered as soon as the particular
sis is established.
ation and Management of
hoproliferative Variant Idiopathic
ophilia
The lymphoproliferative variant of HES is a poorly
number and/or function (Table 2).65 Accordingly, 7 disease
variants are considered, including cutaneous mastocytosis, indo
lent systemic mastocytosis (ISM), SM with an associated clona
hematologic non–mast cell disorder (SM-AHNMD), aggressive
systemic mastocytosis (ASM), mast cell leukemia, mast cel
sarcoma, and extracutaneous mastocytoma.
The WHO classification of mastocytosis mandates a
TABLE 2. WHO Variants of Mastocytosis65
1. Cutaneous mastocytosis (CM)
a. Maculopapular CM
b. Diffuse CM
c. Mastocytoma of skin
2. Indolent systemic mastocytosis (ISM)
a. Smoldering systemic mastocytosis (SSM)
b. Isolated bone marrow mastocytosis
3. Systemic mastocytosis with an associated clonal hematological non–
mast cell lineage disease (SM-AHNMD)
a. SM-myelodysplastic syndrome
b. SM-myeloproliferative disorder
c. SM-chronic eosinophilic leukemia
d. SM-chronic myelomonocytic leukemia
e. SM-non-Hodgkin lymphoma
4. Aggressive systemic mastocytosis (ASM)
With eosinophilia (SM-eo)
5. Mast cell leukemia (MCL)
Aleukemic MCL
6. Mast cell sarcoma
7. Extracutaneous mastocytoma](https://image.slidesharecdn.com/random-130527195759-phpapp02/85/slide-14-320.jpg)
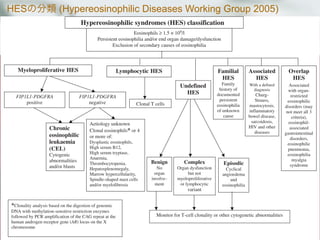
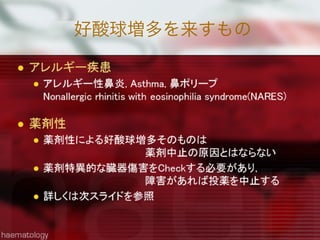
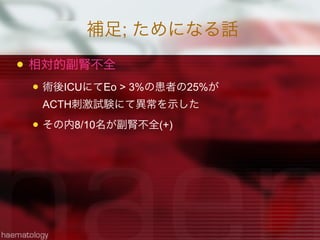
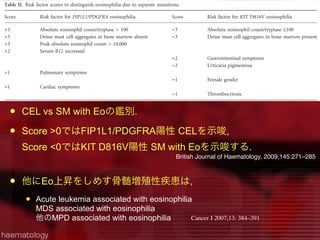
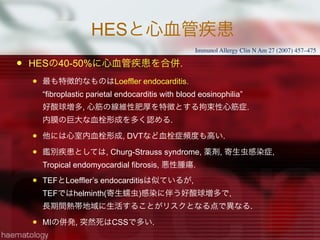
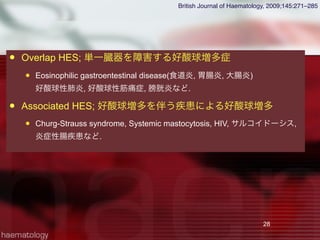
![HES188名のRetrospective study
Baseline;
平均年齢は45yr[6-85], 男性55%.
Fip1-like1-plt-derived growth factor-R α(FP)は11%で陽性
異常T cellは17%で認められ, それらは L-HESと判断.
血清Tryptase値はFP変異陽性群では82%が上昇 vs 20%(非変異群)
血清TARC値はL-HES群で75%上昇 vs 36%(非L-HES群)
HESの臓器症状
臓器症状 初期頻度(%) 全体頻度(%)
皮膚症状 37% 69%
肺障害 25% 44%
消化管障害 14% 38%
心機能障害 <5% 20%
初診時無症状 6%
J Allergy Clin Immunol 2009;124:1319-25](https://image.slidesharecdn.com/random-130527195759-phpapp02/85/slide-21-320.jpg)
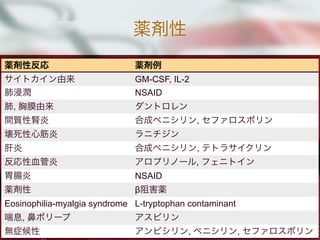
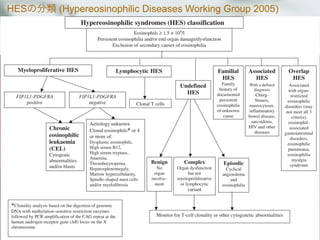
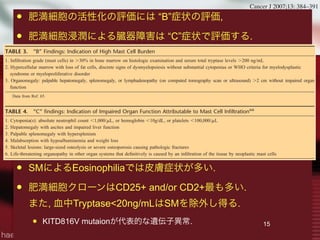
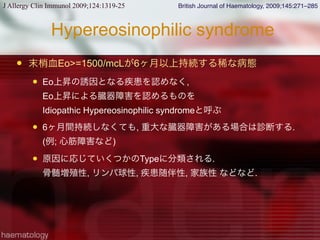
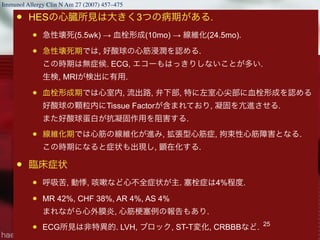
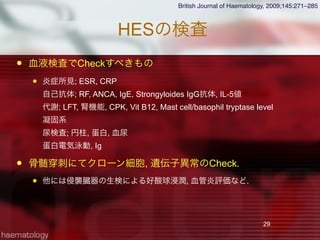
![HESの症状, 侵襲臓器
貧血は53%, PLT低下は31%, PLT増多 16%
骨髄の好酸球増加は33%[7-57]で認められる所見.
米国, 仏, 英の105名の解析.
22
Blood 1994;83: 2759-2779
侵襲臓器 %
心血管 58%
皮膚 56%
神経 54%
肺 49%
脾臓 43%
肝臓 30%
眼 23%
消化管 23%](https://image.slidesharecdn.com/random-130527195759-phpapp02/85/slide-22-320.jpg)
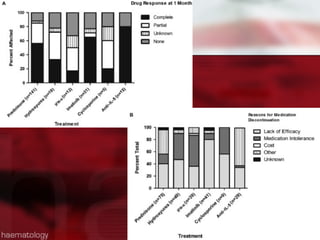
![他の治療
Hydroxyurea 1000mg/d[500-2000]
188名中64名(34%)に使用され, 内18名は単剤治療.
単剤治療群において,
33%で完全寛解, 39%で部分寛解を達成. 副作用での中断は21名
IFN-α 1400万U/wk[300-4000万]
188名中46名(25%)に使用. 12名は単剤治療
単剤治療群において,
17%で完全寛解, 33%で部分寛解を達成.
Cyclosporine 200mg/d[150-500]
Imatinib 400mg/d[100-600]
抗IL-5抗体; Mepolizumab 750mg/mo, Reslizumab 1-3mg/kg/mo](https://image.slidesharecdn.com/random-130527195759-phpapp02/85/slide-32-320.jpg)

This document summarizes causes of eosinophilia, including: 1) It classifies causes of eosinophilia as primary (clonal, idiopathic) or secondary. Secondary causes include infections, tissue invasion by parasites, drugs, allergies, autoimmune diseases, and malignancies. 2) Common primary causes include hypereosinophilic syndrome (HES), chronic eosinophilic leukemia (CEL), and myeloproliferative neoplasms associated with eosinophilia such as those involving FIP1L1-PDGFRA, PDGFRB, FGFR1, and KIT mutations. 3) Secondary causes discussed include parasitic infections, fungal infections, HIV, drugs





































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

