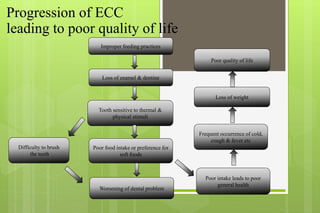
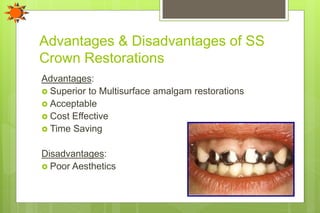
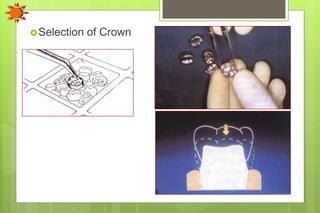
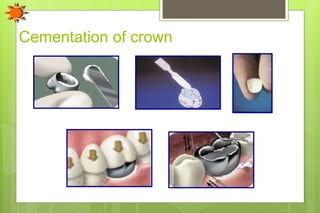
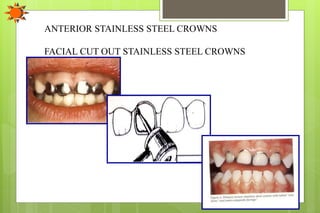
The document discusses the progression of early childhood caries (ECC) leading to poor quality of life. It then summarizes the use of stainless steel crowns in pediatric dentistry, including their introduction, classification based on morphology and composition, indications, advantages, disadvantages, modifications, and complications. Prefabricated stainless steel crowns provide a superior restoration to multi-surface fillings and can help prevent further dental problems if used for extensive decay, following pulp therapy, or as a preventive restoration in primary teeth.














































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



