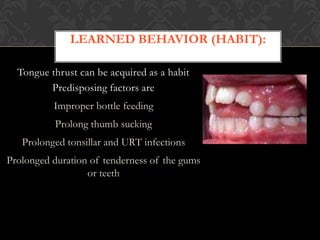
1. Oral habits such as thumb sucking, lip biting, and tongue thrusting are common in children and can persist beyond normal development stages, potentially affecting dental development.
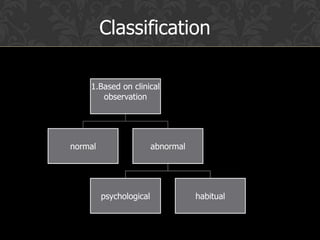
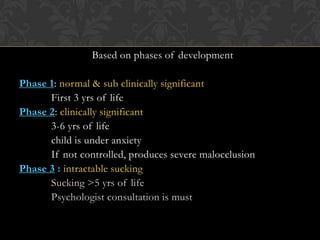
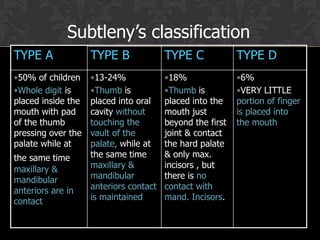
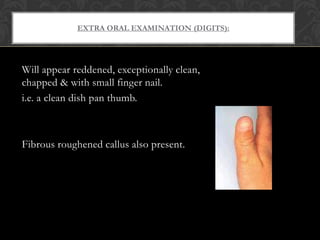
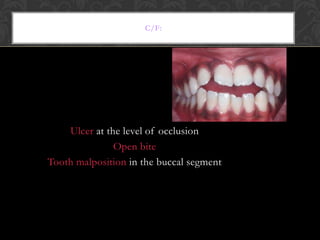
2. Thumb sucking is classified based on factors like intensity, duration, and psychological components, and can cause malocclusion if not addressed.
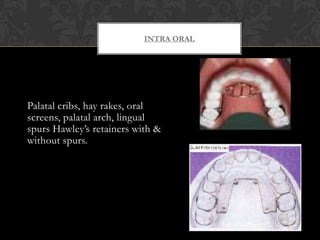
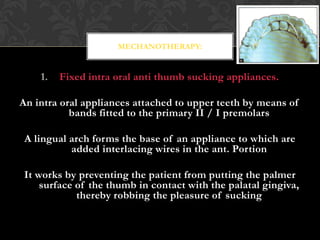
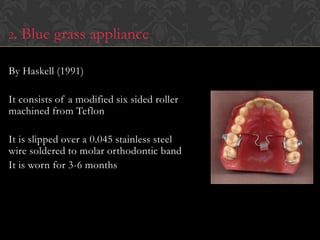
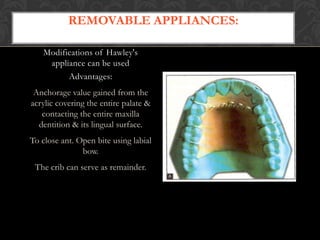
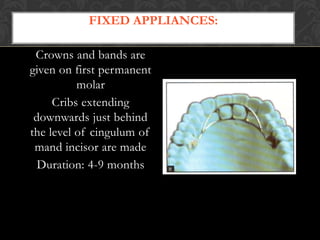
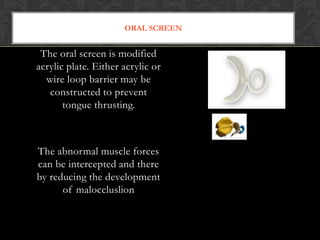
3. Management of oral habits involves psychological therapy, reminder therapy using bitter tastes, and mechanotherapy with intraoral appliances to discourage the habit.