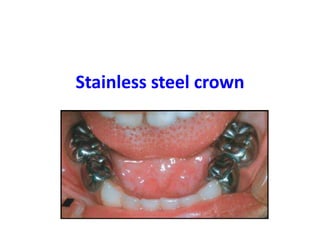
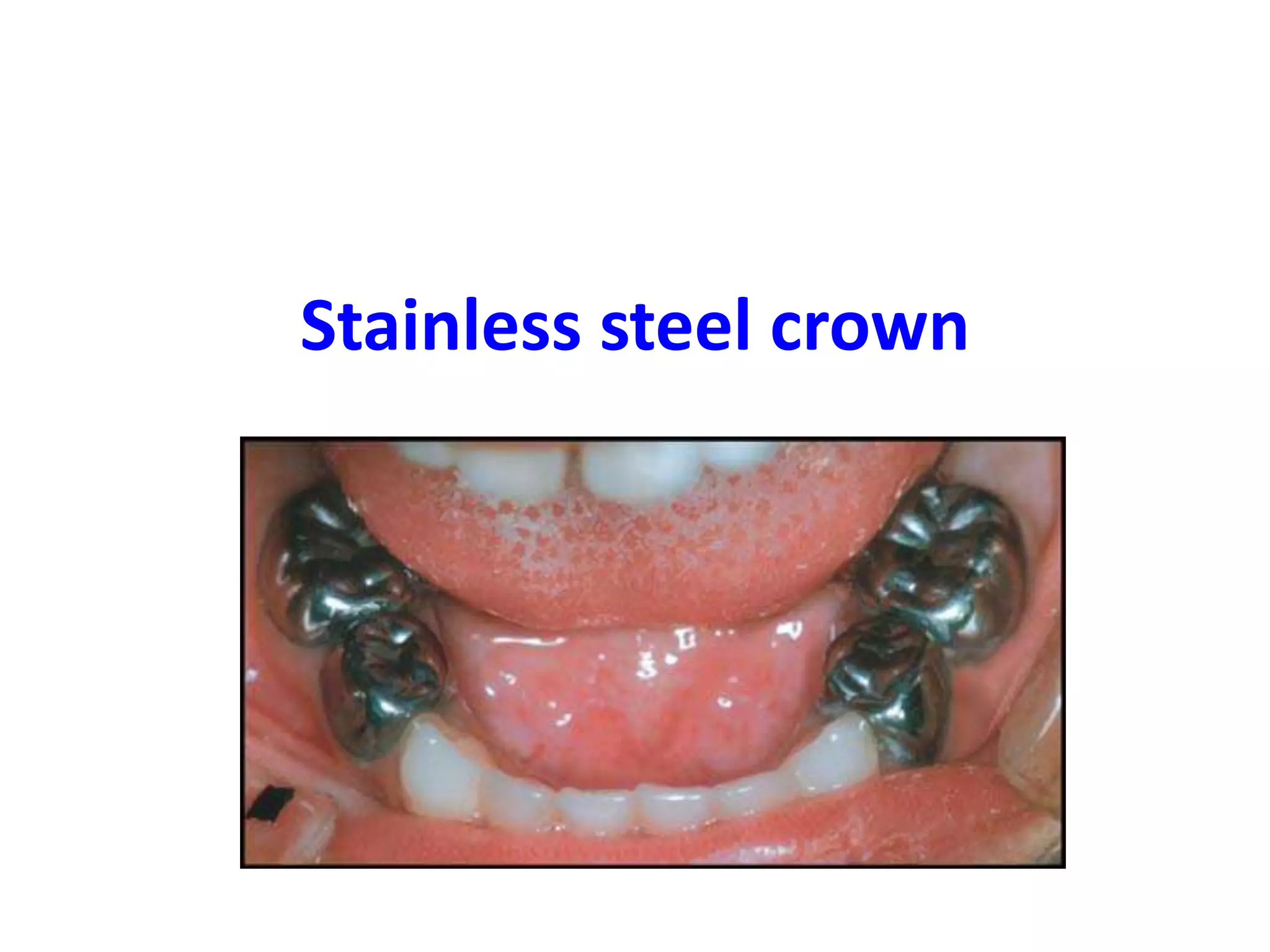
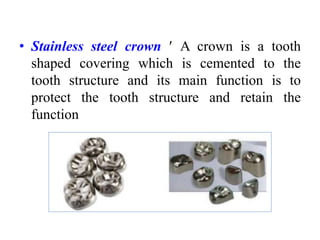
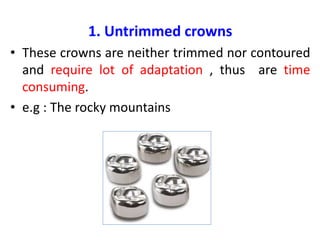
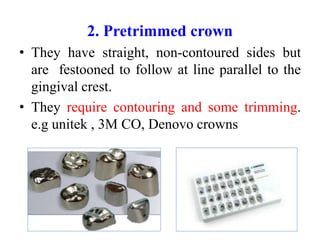
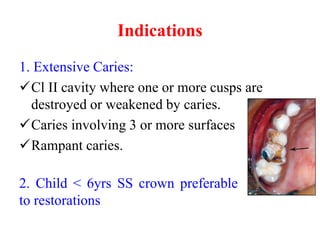
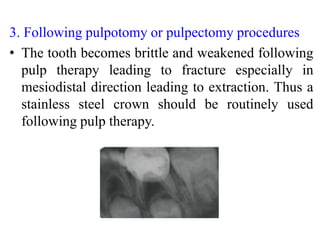
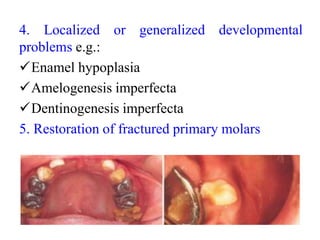
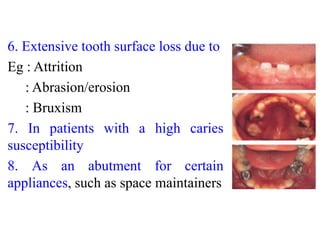
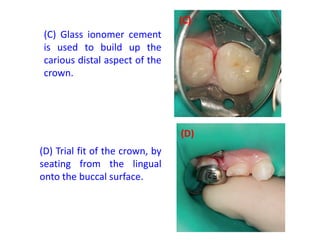
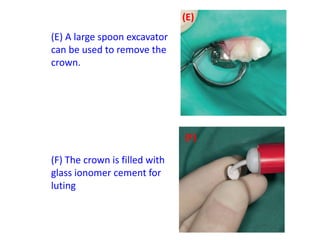
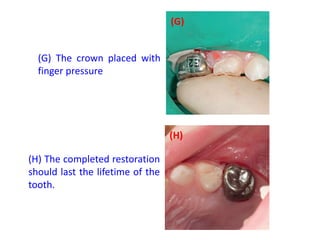
Stainless steel crowns are tooth-shaped coverings cemented onto teeth to protect tooth structure and retain function. They were introduced in 1950 and are commonly used restorations for children and adolescents. They are classified based on composition (e.g. stainless steel, nickel-base) and morphology (untrimmed, pretrimmed, precontoured). Indications include extensive caries, teeth requiring pulpotomy/pulpectomy, developmental defects, and high caries risk. Contraindications include mobile or unerupted teeth. Placement involves tooth preparation, crown selection and fitting, then cementation. The Hall technique places crowns directly over caries with little preparation for cooperative children.




![Classification_of_malocclusion[1] [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/classificationofmalocclusion1read-only-240212164016-9b5c21cb-thumbnail.jpg?width=640&height=640&fit=bounds)
































































