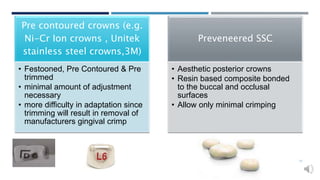
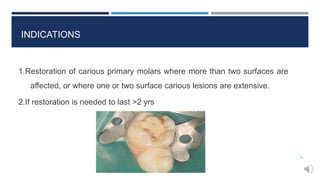
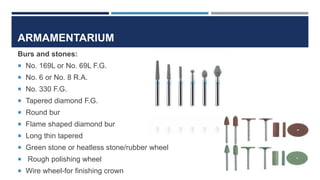
This document provides an overview of stainless steel crowns for pediatric dentistry. It discusses the history, composition, indications, contraindications, advantages and disadvantages of stainless steel crowns. It describes different types of crowns based on composition and morphology. The document outlines the armamentarium, techniques, adaptations and modifications for stainless steel crowns. It is intended to serve as a reference for using stainless steel crowns in treating pediatric dental patients.