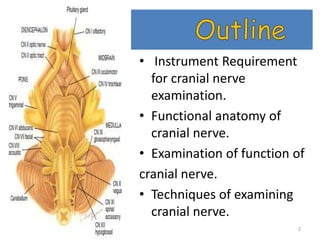
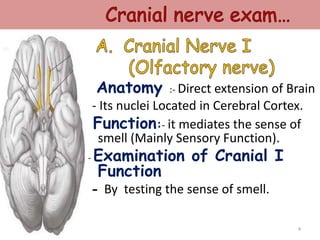
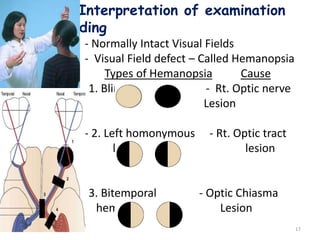
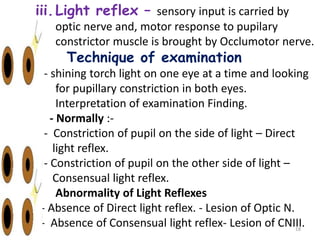
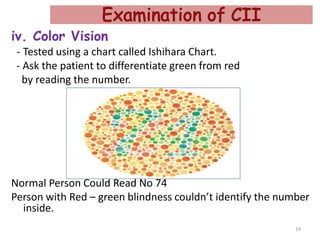
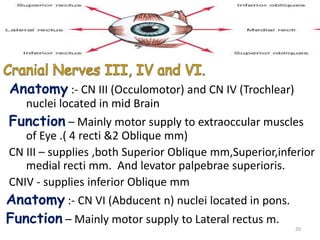
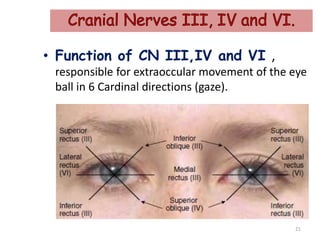
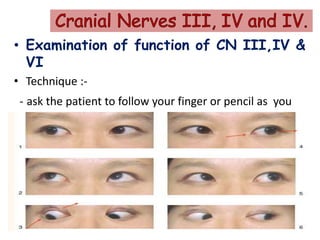
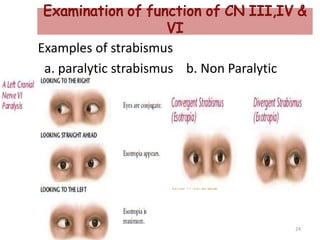
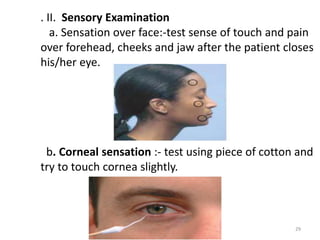
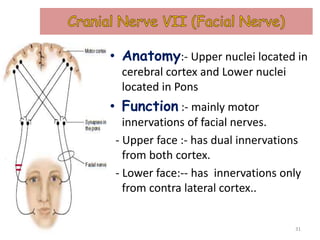
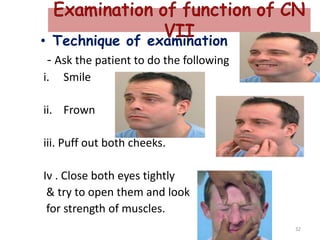
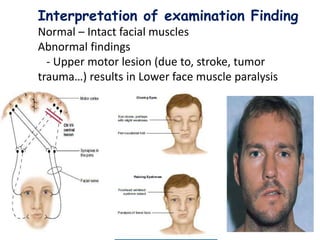
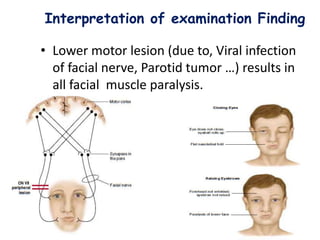
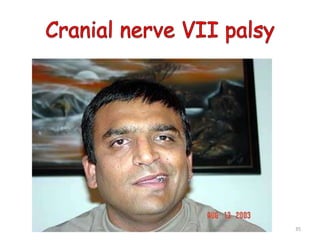
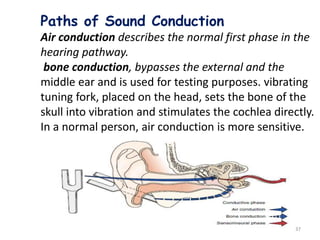
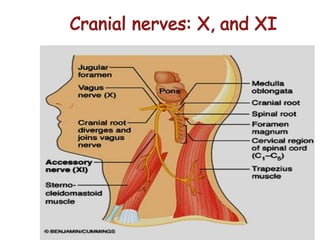
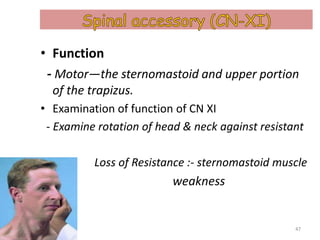
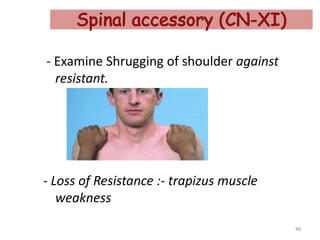
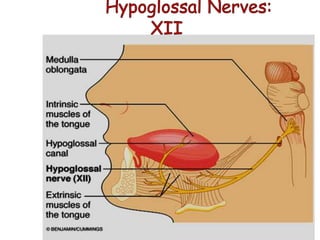
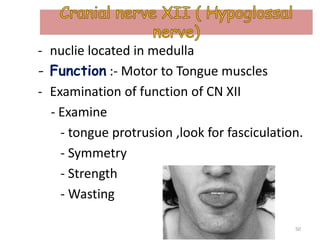
This document provides information on examining the 12 cranial nerves. It discusses the anatomy, function and techniques for examining each nerve. The techniques described include testing smell, visual acuity, visual fields, eye movements, facial expression, hearing, tongue movement, and palate movement. Interpretations of normal and abnormal findings are provided, along with some potential causes of abnormalities.