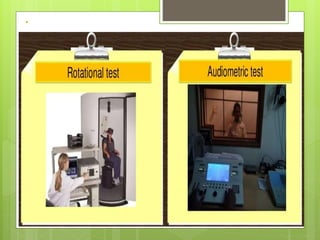
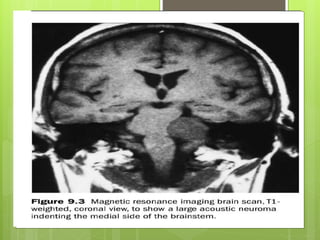
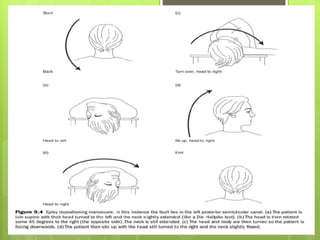
The 8th cranial nerve, also known as the vestibulocochlear nerve, carries sensory information about hearing and balance. It has two divisions - the cochlear nerve for hearing and the vestibular nerve for balance. The nerve exits the brainstem between the pons and medulla and crosses the posterior cranial fossa into the inner ear. Damage to the 8th cranial nerve can cause symptoms like hearing loss, vertigo, and loss of balance. Tests like the caloric test and Dix-Hallpike maneuver examine the vestibular component, while audiometry tests the cochlear component. Treatment may include rest, medications, exercises, or surgery to relieve severe symptoms.

![Vestibulocochlear nerve VIII
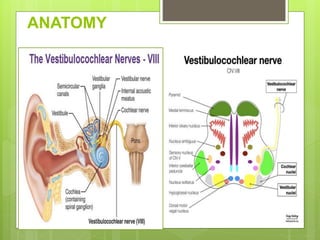
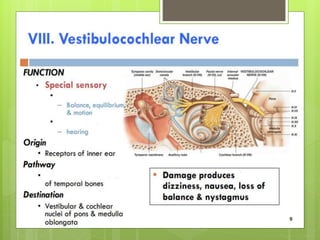
•ANATOMY
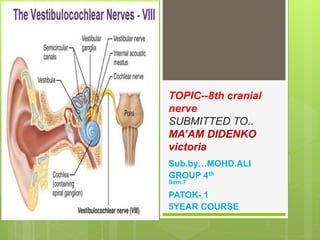
The vestibulocochlear nerve [VIII] carries SA fibers for hearing
and balance,
consists of two divisions:
1. A Vestibular component for balance.
2. A Vochlear component for hearing.
1.The vestibulocochlear nerve
attaches to the lateral surface of the brainstem,
between the pons and medulla,
after emerging from the internal acoustic meatus and
crossing the posterior cranial fossa into the single nerve seen
in the posterior cranial fossa within the substance of the
petrous part of the temporal bone](https://image.slidesharecdn.com/ali8cranialnerve-211124112242/85/cranial-nerve-3-320.jpg)