This document summarizes the anatomy and physiology of equilibrium. It discusses:
1) The functions of equilibrium include general body orientation, balanced locomotion, readjusting autonomic functions after reorientation, and gaze stabilization.
2) These functions are achieved through vestibulo-ocular reflex, vestibulospinal reflex, and vestibulosympathetic reflex.
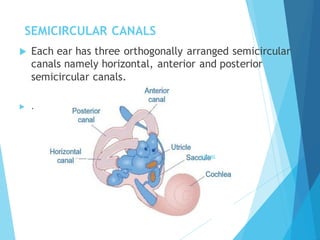
3) The receptors for movement detection are the semicircular canals and otolith organs within the vestibular labyrinth of each inner ear.















































![Radiological anatomy of_temporal_bone[1]](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicalanatomyoftemporalbone1-171112100915-thumbnail.jpg?width=640&height=640&fit=bounds)

























































