Coronavirus disease 2019(covid 19)
•Download as PPTX, PDF•
11 likes•1,017 views

COVID-19 is a global infectious disease pandemic with high morbidity and mortality for at risk individuals. This slide is intended for the medical students, medical doctors and those in training for masters of medicine (MMED).

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Coronavirus disease 2019(covid 19)
Similar to Coronavirus disease 2019(covid 19) (20)
Recently uploaded
Recently uploaded (20)
Coronavirus disease 2019(covid 19)
- 2. Outline i. Introduction ii. Epidemiology iii. Pathogenesis iv. Clinical presentation v. Diagnosis. vi. Pharmacology of the drugs used for treatment of COVID-19
- 3. Introduction • Coronaviruses are important human and animal pathogens (zoonoses). • Together with other zoonoses, this disease form group of emerging and reemerging zoonoses • At the end of 2019, a novel coronavirus was identified as the cause of a cluster of pneumonia cases in Wuhan, a city in the Hubei Province of China. • It rapidly spread, resulting in an epidemic throughout China, with sporadic cases reported globally. • In February 2020, the WHO designated the disease COVID-19, which stands for coronavirus disease 2019.
- 4. Cont.. • The virus that causes COVID-19 is designated severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2); previously, it was referred to as 2019-nCoV, this large viruses containing a single-stranded positive-sense RNA genome enveloped by a membrane. • The disease spread throughout the world and on 11th March 2020, WHO declared it as the pandemic. • To date, there are no SARS-CoV-2-specific antiviral agents, most of the drugs used for treatment are used for treatment of other infectious disease.
- 5. Epidemiology • The worlwideCOVID-19 statistics as of 22nd May 2020 i. Total confirmed cases: 5.11million ii. Death: 333,001 (6.5%) iii. Recovered: 1.95 million(38.2%) iv. Currently infected patients: 2.83 million (55.3%) • The United Republic of Tanzania reported its 1st case of COVID-19 on 16th March 2020
- 6. Cont… • Epidemiologic investigation in Wuhan at the beginning of the outbreak identified an initial association with a seafood market that sold live animals, where most patients had worked or visited and which was subsequently closed for disinfection. • However, as the outbreak progressed, person-to-person spread became the main mode of transmission. • ?? The origin of the virus still possess a lot of questions as there have been reports that It may have originated from the labs at the Wuhan Institute of Virology and then spread to the community
- 7. Cont.. • Person-to-person spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is thought to occur mainly via respiratory droplets, resembling the spread of influenza. • With droplet transmission, virus released in the respiratory secretions when a person with infection coughs, sneezes, or talks can infect another person if it makes direct contact with the mucous membranes; infection can also occur if a person touches an infected surface and then touches his or her eyes, nose, or mouth.
- 8. Cont.. • The incubation period of COVID-19 ranges between 2- 14 days, about 80% of the patients will show no/mild symptoms but they are potential source of viral transmission to other individuals • According to the WHO, recovery time appears to be around two weeks for mild infections and three to six weeks for severe disease. • People with advanced age, with Comorbidities such as HIV, D. mellitus, cancer, Heart failure, Obesity and CKD have increased morbidity and mortality
- 9. Pathogenesis • Patients with COVID-19 show clinical manifestations including fever, nonproductive cough, dyspnea, myalgia, fatigue, normal or decreased leukocyte counts, and radiographic evidence of pneumonia that includes ground glass opacification. • Although the pathogenesis of COVID-19 is not wholly understood, the knowledge of SARS-COV & MERS-COV pathogenesis and available data on SARS-CoV-2 give an insight to the current knowledge • In ~ 80% of the infected patients, the disease will be mild and mostly restricted to the upper and conducting airways.
- 10. Cont.. • Preliminary reports suggested that the reproductive number (R₀), the number of people who acquire the infection from an infected person, was estimated to be 2.2 to 3.3. • However, the R₀ may actually be lower in light of social distancing measures that have been instituted. • The secondary attack rate for SARS-CoV-2 is estimated to be 0.45% for close contacts of US patients.
- 11. Virology • This is an intracellular microorganism • Coronaviruses (CoVs) are relatively large viruses containing a single-stranded positive-sense RNA genome encapsulated within a membrane envelope. • The viral membrane is studded with glycoprotein spikes that give coronaviruses their crownlike appearance. • There are four classes of coronaviruses designated as alpha, beta, gamma, and delta.
- 12. Cont… • the evidence from the phylogenetic analysis indicates that the COVID-19 belongs to the genus betacoronavirus, which includes SARSCoV, that infects humans, bats, and wild animals • The betacoronavirus class includes: i. Severe acute respiratory syndrome (SARS) virus (SARS-CoV) ii. Middle East respiratory syndrome (MERS) virus (MERS-CoV) iii. COVID-19 causative agent SARS-CoV-2 (with has 85% genetic homology with SARS-CoV)
- 13. Cont… • Similar to SARS-CoV and MERS-CoV, SARS-CoV-2 attacks the lower respiratory system to cause viral pneumonia, but it may also affect the gastrointestinal system, heart, kidney, liver, and central nervous system leading to multiple organ failure. • Evidences indicates that SARSCoV-2 is more contagious than SARS-CoV
- 14. Cont… • SARS-CoV2 genome encodes several structural proteins, including the glycosylated spike (S) protein that functions as a major inducer of host immune responses. • This S protein mediates host cell invasion by both SARS-CoV and SARS-CoV-2 via binding to a receptor protein called angiotensin-converting enzyme 2 (ACE2) located on the surface membrane of host cells. • The invasion process requires S protein priming which is facilitated by the host cell produced serine protease TMPRSS211.
- 16. Cont.. • In addition, the viral genome also encodes several nonstructural proteins including RNA-dependent RNA polymerase (RdRp), coronavirus main protease (3CLpro), and papain-like protease (PLpro). • Upon entrance to the host cells, the viral genome is released as a single-stranded positive RNA. Subsequently, it is translated into viral polyproteins using host cell protein translation machinery, which are then cleaved into effector proteins by viral proteinases 3CLpro and PLpro.
- 17. Cont… • PLpro also behaves as a deubiquitinase that may deubiquinate certain host cell proteins, including interferon factor 3 and NF-κB, resulting in immune suppression. • RdRp synthesizes a full-length negative-strand RNA template to be used by RdRp to make more viral genomic RNA.
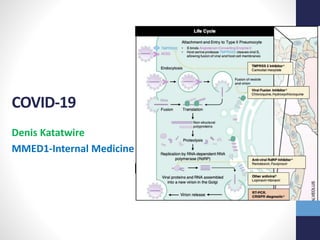
- 18. Coronavirus entry and replication • The inhaled virus SARS-CoV-2 likely binds to epithelial cells in the nasal cavity and starts replicating, Coronavirus S protein is regarded as a major determinant of virus entry into host cells. • The envelope spike glycoprotein binds to its cellular receptor, ACE2 for SARS-CoV and SARS-CoV-2 , CD209L(a C-type lectin, also called L-SIGN) for SARS-CoV, DPP4 for MERS-CoV. • The virus propagates and migrates down the respiratory tract along the conducting airways, and a more robust innate immune response is triggered.
- 19. Cont… • The entry of SARS-CoV into cells was initially identified to be accomplished by direct membrane fusion between the virus and plasma membrane however it has been identified that critical proteolytic cleavage event occurs at SARS-CoV S protein at position (S20) mediating the membrane fusion and viral infectivity. • Besides membrane fusion, the clathrin-dependent and - independent endocytosis mediate SARS-CoV entry too. • Upon entry, the viral RNA genome is released into the cytoplasm and is translated into two polyproteins and structural proteins resulting into subsequent viral genome replication.
- 20. Cont… • The newly formed envelope glycoproteins are inserted into the membrane of ER or Golgi, and the nucleocapsid is formed by the combination of genomic RNA and nucleocapsid protein (post-translational modification). • Then, viral particles germinate into the endoplasmic reticulum-Golgi intermediate compartment (ERGIC). At last, the vesicles containing the virus particles then fuse with the plasma membrane to release the virus
- 22. Antigen presentation in coronavirus infection • Presentation to the antigen presentation cells(APCs) is a central part of the body’s anti-viral immunity. • Antigenic peptides are presented to the MHC/HLA and then recognized by virus-specific cytotoxic T lymphocytes (CTLs) which is important in comprehension of COVID-19 pathogenesis. • The antigen presentation of SARS-CoV depends mostly on MHC I molecules however MHC II molecules plays a role.
- 23. Cont.. • HLA-B*4601, HLA-B*0703, HLA-DR B1*1202 and HLA- Cw*0801 genetic polymorphism have been associated with increased susceptibility to SARS infection, on the other hand HLA-DR0301, HLA-Cw1502 and HLA-A*0201 alleles offers protection from SARS infection. • Genetic polymorphisms of MBL (mannose-binding lectin) associated with antigen presentation are related to the risk of SARS-CoV infection.
- 24. Humoral and cellular immunity • Antigen presentation results in stimulation of both humoral and cellular immunity as the consequence of activation of virus-specific B and T cells. • Similar to common acute viral infections, the antibody profile against SARS-CoV virus has a typical pattern of IgM and IgG production.
- 25. Cont… • SARS-specific IgM antibodies disappear at the end of week 12, while the IgG antibody last for a long time, which indicates IgG antibody may play a protective role, and the SARS-specific IgG antibodies primarily are S-specific and Nspecific antibodies. • The most important cellular immunity response is the significant reduction in CD4+ and CD8+ T cells in the peripheral blood of SARS-CoV-2-infected patients (similar to SARS-CoV) due to their excessive activation.
- 26. Cont.. • The interaction between viral S protein and ACE2 on the host cell surface is of significant interest since it initiates the infection process, the binding affinity of SARS-CoV-2 S protein to ACE2 is about 10-20 times higher than that of SARS-CoV S protein. • It is speculated that this may contribute to the reported higher transmissibility and contagiousness of SARS-CoV-2 as compared to SARS-CoV.
- 27. Cont… • ACE2 involvement with coronavirus infection is of further interest since ACE2 is a potent negative regulator restraining overactivation of RAAS (renin angiotensin aldosterone system) that may be involved in elicitation of inflammatory lung disease in addition to its well-known role in regulation of blood pressure and balance of body fluid and electrolytes. • Organs considered to be more vulnerable to SARS-CoV-2 infection due to their ACE2 expression levels include pneumocytes type II of the lungs, heart, oesophagus, kidneys, bladder, and ileum
- 28. Cont • ACE2 enzyme catalyzes degradation of angiotensin II to angiotensin (1-7). • The balance between angiotensin II and angiotensin (1-7) is critical since angiotensin II binds to angiotensin receptor (AT1) to cause vasoconstriction, whereas angiotensin (1-7) elicits vasodilation mediated by AT2. • The chronic activation of ACE2 as a result of SARS-CoV-2 infection culminate in its downregulation which impair its physiological functions resulting in pulmonary vascular constriction and worsening hypoxemia
- 29. Cytokine storm in COVID-19 • ARDS is the main cause of death COVID-19. • ARDS is the common immunopathological event for SARS- CoV-2, SARS-CoV and MERS-CoV infections, it’s major mechanism being the cytokine storm; the deadly uncontrolled systemic inflammatory response resulting from the release of large amounts of pro-inflammatory cytokines (IFN-a, IFN-g, IL- 1b, IL-6, IL-12, IL-18, IL-33, TNF-a, TGFb, etc.) and chemokines (CCL2, CCL3, CCL5, CXCL8, CXCL9, CXCL10, etc.) by immune effector cells in SARS-CoV/ SARS-CoV-2 infection.
- 30. Cont.. • The cytokine storm trigger a aggressive attack by the immune system to the body resulting into ARDS and multiple organ failure, and finally lead to death in severe cases of SARS-CoV-2 infection, just like what occurs in SARS-CoV and MERSCoV infection. • The cytokine storm results in activation of endothelium and subsequent endothelial dysfunction culminating in excess thrombin generation and fibrinolysis shutdown which cause a hypercoagulable state, overt DIC occur in patients in later stages of COVID-19 infection, while still hospitalized, often with septic physiology and multiorgan failure.
- 31. Cont.. • In addition, the hypoxia found in severe COVID-19 can stimulate thrombosis through not only increasing blood viscosity, but also a hypoxia-inducible transcription factor- dependent signaling pathway. • Polyphosphates, derived from microorganisms, activates platelets, mast cells, and FXII in the contact pathway of coagulation, and exhibit other downstream roles in amplifying the procoagulant response of the intrinsic coagulation pathway. Complement pathways also contribute to activation of coagulation factors.
- 32. Cont.. • Occlusion and microthrombosis formation in pulmonary small vessels of critical patient with COVID-19 has been reported from a recent lung organ dissection therefore early application of anticoagulant therapy in severe COVID-19 have been suggested in bid to improve outcome. • Coagulopathy of COVID-19 presents with prominent elevation of D-dimer and fibrin/fibrinogen degradation products, while abnormalities in prothrombin time, partial thromboplastin time, and platelet counts are relatively less pronounced making it different from DIC.
- 33. Viral load and shedding • High viral loads have been detected in nasal and throat swabs soon after symptom onset, asymptomatic patients may have similar viral load compared with symptomatic patients. • Pharyngeal viral shedding is high during the first week of symptoms when symptoms are mild or prodromal, peaking on day suggesting active virus replication in upper respiratory tract tissues. • Duration of viral shedding is between 8 and 20 days after symptoms resolution, virus can be detected in the sputum and faeces for up to 39 days after negative pharyngeal swabs, it is not clear if this phenomenon results in transmission of virus. • Factors associated with prolonged viral shedding include male sex, older age, comorbid hypertension, delayed admission to hospital after symptom onset or severe illness on admission, and use of invasive mechanical ventilation or corticosteroids.
- 34. Coronavirus immune evasion • Multiple strategies are used by these viruses to avoid immune responses. i. Normally the evolutionarily conserved microbial structures called pathogen-associated molecular patterns (PAMPs) are recognized by pattern recognition receptors (PRRs) however these viruses can induce production of double-membrane vesicles which do not contain PRRs and then replicate in these vesicles, thereby avoiding the host detection of their dsRNA. ii. IFN-I has protective effects in infection with these viruses however its production is inhibited rendering them capable of evading the immune system iii. Down regulation of gene expression related to antigen presentation
- 35. ??Why now…??Why not always Zoonotic Evolution and Adaptation • Quick rate of replication and reproduction in the background of lacking Proof reading mechanisms = accumulation of mutations. E.g. HIV-1 virus is thought to be the world’s fastest evolving microbe (Cuevas et al, 2015). • ?2002 China’s Guangdong twenty-first century’s first global pandemic: SARS due to SARS-CoV = acquired two key mutations in the receptor-binding domain of its S protein that allowed it to use the human orthologue of the receptor ACE2 with high efficiency. The mutations enabled SARS-CoV to jump from its natural reservoir which is bats into civets then to human resulting into the outbreak. • Seems to be the similar case for COVID-19 due to SARS-CoV2
- 36. ??Bioterrorism • Conspiracy theorists have suggests that COVID-19 was planned and the causative virus was created/manipulated in the laboratory • However SARS-COV-2 have 85% genetic homology with SARS- COV, 50% to the MERSCoV and since zoonotic disease are difficult to predict this may explain the normal process of zoonotic evolution. • Evidence from phylogenetic analysis shows that the virus was not manipulated/manufactured in the laboratory
- 37. Clinical presentation of COVID-19 • The most common symptoms at onset of COVID-19 illness are fever, cough, fatigue and anosmia as the disease progress the patient develop sputum production, headache, haemoptysis, diarrhoea, dyspnoea, and lymphopenia. • Clinical features revealed by a chest CT scan presents as pneumonia, however, there were abnormal features such as RNAaemia, acute respiratory distress syndrome, acute cardiac injury (myocarditis), and incidence of grand-glass opacities that led to death.
- 38. Clinical course/natural hx of COVID-19 • Out of population of individuals who develop COVID-19, 80% develop mild or no symptoms but are very infectious, therefore they can be isolated and treated at home. • About 20% develops moderate to severe symptoms with pulmonary infiltrates and some of these will develop very severe disease. • About 5-10% develop severe symptoms with ARDS, Sepsis, multiorgan failure and coagulopathy necessitating admission into an ICU.
- 39. WHO classification i. Mild illness (Upper respiratory tract symptoms) ii. Moderate illness (Pneumonia) iii. Severe illness (severe pneumonia, sepsis, septic shock and multiorgan failure)
- 41. Diagnosis • Thorough hx taking P.Examination: The respiratory clinical manifestations consistent with COVID-19 (eg, fever, cough, dyspnea). Symptomatic patients should also be asked about recent travel or potential COVID-19 exposure in the prior 14 days to determine the need for evaluation for COVID-19. • RNA PCR (RT-PCR) & Viral genetic sequencing • Viral specific IgM & IgG titres • Radiography..CXR (hazy bilateral , peripheral opacities), CT Chest (GGO, consolidation, rarely may be unilateral), USS: numerous B-lines, pleural line thickening, consolidation with air bronchograms
- 42. Labs • CBC: leukopenia & lymphopenia (>80%) • RFT: Increased BUN/Cr • LFT: Increased ASAT/ALAT/Total bilirubin • Increased D-dimer, CRP, LDH • Increased IL-6, Ferritin • Low levels of procalcitonin, high levels Procalcitonin suggests concurrent bacterial superinfection
- 43. Treatment of COVID-19 • Some patients with suspected or documented COVID-19 have severe disease that warrants hospital care. • Since there is limited clinical and basic research information at this time, treatment options for COVID-19 currently comprise investigational drugs and management of symptoms. • Ensuring appropriate infection control and supportive care. • High-flow oxygen and noninvasive positive pressure ventilation, Acute respiratory distress syndrome warrant intubation with mechanical ventilation; extracorporeal membrane oxygenation may be indicated in patients with refractory hypoxia, the aim is SPO2 >_94%
- 44. Cont.. • The WHO and CDC recommend against the use of glucocorticoids in patients with COVID-19 pneumonia unless there are other indications (eg, exacerbation of chronic obstructive pulmonary disease (COPD)). • Glucocorticoids have been associated with an increased risk for mortality in patients with influenza and delayed viral clearance in patients with MERS-CoV and SARS-CoV. • Most drugs for the treatment of COVID-19 are still under clinical trials and since most of the same are safe and have demonstrated efficacy, they are used for the purpose of COVID-19
- 45. Cont.. • Anticoagulation therapy early after admission for eligible patients. • Antimicrobial therapy for treatment of suspected bacterial infection should be instituted based on the local guidelines, clinical presentation and susceptibility pattern until blood culture can rule out the infection. • Use of the convalescent plasma of the recovered patients • Use of intravenous Vitamin C • Physiotherapy that includes chest physiotherapy; avoid lying on their back as this makes coughing ineffective and chest physiotherapy
- 47. Chloroquine/Hydroxychloroquine +/- Azithromycin • The sulfate and phosphate salts of chloroquine have both been commercialized as antimalarial drugs. • Hydroxychloroquine has also been used as an antimalarial, but in addition is now broadly used in autoimmune diseases such as lupus and rheumatoid arthritis. • Of note, chloroquine and hydroxychloroquine are considered to be safe and side-effects are generally mild and transitory. • However, the margin between the therapeutic and toxic dose is narrow and chloroquine poisoning can be life threathening.
- 48. Cont.. • MOA: increasing endosomal pH required for virus/cell fusion, as well as interfering with the glycosylation of cellular receptors of SARS-CoV2 . The anti-viral and anti-inflammatory activities of chloroquine may account for its potent efficacy in treating patients with COVID-19 pneumonia. • Chloroquine is a cheap and safe drug that has been used for more than 70 years. In light of the urgent clinical demand, chloroquine phosphate is recommended to treat COVID-19 associated pneumonia in larger populations in the future. • Safety concerns with hydroxychloroquine and azithromycin include the potential for QTc prolongation, which is greater when both agents are used together and may accounted for increased mortality reported in some clinical trials.
- 51. Remdesivir • =Novel antiviral drug developed for the treatment of Ebola virus disease and Marburg virus infections. • It is a prodrug of a nucleotide analog that is intracellularly metabolized to an analog of adenosine triphosphate that inhibits viral RNA polymerases. • Remdesivir has broadspectrum activity against members of several virus families, including filoviruses (e.g., Ebola) and coronaviruses e.g., SARSCoV and MERSCoV). • In vitro testing has also shown that Remdesivir has activity against SARS-CoV-2 with an EC50 value of 1.76 μM
- 52. Cont • The discussed drugs (specifically Chloroquine /Hydroxychloroquine and Remdesivir ) have shown improvement of symptoms and severity of the COVID-19 disease, however the their ability to improve mortality in these patients remain inconclusive and require further clinical trials involving large number of participants to reach such conclusion
- 53. Prevention In the health care setting • Screening and precautions for fever or respiratory symptoms — Screening patients for clinical manifestations consistent with COVID-19 (eg, fever, cough, dyspnea) prior to entry into a health care facility can help identify those who may warrant additional infection control precautions. Symptomatic patients should also be asked about recent travel or potential COVID- 19 exposure in the prior 14 days to determine the need for evaluation for COVID-19. • Any individual with these manifestations should wear a facemask. • PPE for healthcare workers
- 54. Management in Pregnancy & Paediatrics • Pregnant women should be managed by a multidisciplinary team, including obstetric, perinatal, neonatal, and intensive care specialists, as well as mental health and psychosocial support. There is no evidence to suggest that pregnant women are more likely to contract COVID-19, or present with increased risk of severe illness or fetal compromise. • Mothers in labour/not in labour with suspected/confirmed COVID-19 should isolated from the general wards , being in room containing patients each! • IPC guidelines should be adhered
- 55. • All other treatment should be done as indicated, delivery should be conducted with other indications as COVID-19 infection is not an indication for delivery..the fetus is unlikely to be infected during pregnancy • When the mother has confirmed COVID-19: after delivery of healthier baby should cared separately by a relative/caregiver and must be tested for COVID-19. • When with signs and symptoms of COVID-19 a baby should admited into the NICU unless the symptoms are mild and managed separately under care of Neonatologist . • Other group of paediatric patients should managed with the same protocol as adults however the drug doses and fluid management should be adjusted accordingly. Cont…
- 56. Cont… • WHO recommends standard, contact, and droplet precautions (i.e., gown, gloves, and mask), with eye or face protection. • The CDC recommends that patients with suspected or confirmed COVID-19 be placed in a single-occupancy room with a closed door and dedicated bathroom. The patient should wear a facemask if being transported out of the room (eg, for studies that cannot be performed in the room). • Adhering to Infection Prevention and Control Protocol.
- 57. Cont.. Preventing exposure in the community • Diligent hand washing, particularly after touching surfaces in public. Use of hand sanitizer. • Respiratory hygiene (eg, covering the cough or sneeze). • Avoiding touching the face (in particular eyes, nose, and mouth). • Screening and Quarantine of the contacts and travelers from high risk geographical location • Social distancing • Cleaning and disinfecting objects and surfaces that are frequently touched. • Shielding extremely vulnerable people
- 58. Vaccine • It is crucial to develop safe and effective vaccines to control the COVID-19 pandemic, eliminate its spread, and ultimately prevent its future recurrence. • Since the SARS-CoV-2 virus shares significant sequence homology with two other lethal coronaviruses, SARS and MERS, the vaccines identified in these patents related to SARS and MERS viruses could potentially facilitate the design of anti-SARS-CoV-2 vaccines.
- 59. Cont... • There is currently no vaccine for SARS-CoV2 however many vaccines are undergoing clinical trials though others are still in the animal phase and this may take up to another 12 months to have at least one vaccine. • The viral S protein subunit vaccines have been shown to produce higher neutralizing antibody titers and more complete protection than live-attenuated SARS-CoV, full- length S protein, and DNA-based S protein vaccines.
- 60. Prognosis • The following are associated with increased likelihood of poor clinical outcome: i. Advanced age ii. Comorbidities: DM, COPD, Asthma, CVD, Obesity iii. High SOFA score at admission iv. Admission to the ICU v. Labs findings: high levels of D-dimer, ferritin, troponin, cardiac myoglobin vi. Watch for complications such as secondary bacterial infection, stress CM
- 61. What is next for COVID-19? • COVID-19 does not yet have specific therapy! • Individuals should adapt to live with the virus as cure will not attained unless proper therapy is identified, 70% of the population is infected and thus attaining herd immunity ( this is not yet scientifically proven) and the safe and efficient vaccine is developed. • ?? There is likelihood of this disease developing 2nd/3rd ….. wave that may be more severe than what we have experienced so far.
- 62. Questions 1. Distinguish suspected case from confirmed case of COVID- 19, How does their management differs? 2. Explain the major routes of transmission of SARS-CoV-2 3. Keeping in mind the Role of ACE2 receptor in pathogenesis of COVID-19 in mind, should the patients on ACEIs/ARBs be withheld? Explain you answer! 4. Use of Glucocorticoids are limited in these patients, when would the continuation of steroid therapy be mandatory? Which form of steroid therapy should not be withheld? 5. What are major causes of death in COVID-19 patients? 6. What is drug repurposing? When is it important? 7. What is the role of convalescent plasma in Management of COVID-19?
- 63. Cont.. 8. Can Chloroquine/Hydroxychloroquine be used as prophylaxis against SARS-CoV-2? What gives this drug this property? How is it safe and efficacious? 9. Where can the samples for RT-PCR testing be taken?? What are their sensitivity and specificity? 10. What are the roles of different types of face masks in prevention of COVID-19?? 11. Discuss the role and timing of lockdown in prevention of COVID-19 and its implication on social-economic aspects of different societies 12. What are complications of COVID-19? Explain how they can be managed!
- 64. Case scenario • A 73-year-old man with hypertension and chronic obstructive pulmonary disease calls to report that he has had a fever (maximal temperature, 38.3°C) and a dry cough for the past 2 days. He notes that his shortness of breath has worsened. His medications include losartan and inhaled glucocorticoids. He lives alone. How should he be evaluated? If he has coronavirus disease 2019 (Covid-19), the disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), then how should he be treated?
- 65. References • Notification of 2019-nCoV infection. National Health Commission of the People's Republic of China. http:// www.nhc.gov.cn/xcs/yqfkdt/202002/18546da875d74445b b537ab014e7a1c6.shtml (accessed February 17, 2020). (in Chinese) • Hussin A. Rothan and Siddappa N. Byrareddy, Journal of Autoimmunity, https://doi.org/10.1016/j.jaut.2020.102433 • https://www.covid19treatmentguidelines.nih.gov/ • Mason RJ. Pathogenesis of COVID-19 from a cell biology perspective. Eur Respir J 2020; 55: 2000607 [https://doi.org/10.1183/13993003.00607-2020]
- 66. References • X. Li et al, Molecular immune pathogenesis and diagnosis of COVID-19, https://doi.org/10.1016/j.jpha.2020.03.001 • Jianjun Gao, Zhenxue Tian, Xu Yang; Breakthrough: Chloroquine phosphate has shown apparent efficacy in treatment of COVID-19 associated pneumonia in clinical studies • Caren G. Solomon, M.D., M.P.H., Mild or Moderate Covid-19, DOI: 10.1056/NEJMcp2009249. • Parag Goyal, M.D et al, Clinical Characteristics of Covid-19 in New York City, DOI: 10.1056/NEJMc2010419 • CDC Guidelines on COVID-19 • WHO Guidelines on COVID-19