Downloaded 107 times

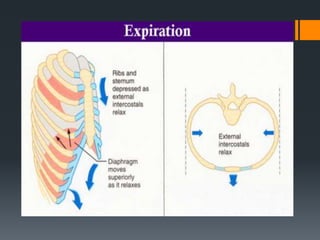





This document discusses control of breathing. It begins by defining breathing and respiration, noting that breathing is the process of inhaling and exhaling air while respiration involves cellular oxidation reactions. It then describes the mechanics of breathing, including inspiration driven by diaphragm and intercostal muscle contraction, and expiration triggered by relaxation of these muscles. The document outlines three levels of nervous control over breathing: primary control by the medulla oblongata in response to rising blood CO2 and H+ levels, secondary control via chemoreceptors responding to blood O2, and alveolar control through stretch receptors signaling full alveoli to the medulla.































































































