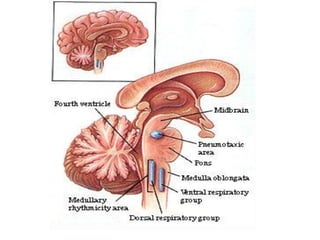
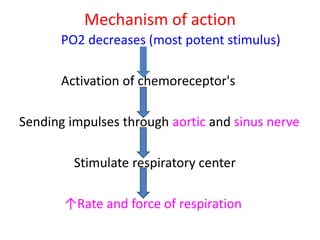
The document summarizes the regulation of respiration through nervous and chemical mechanisms. The nervous mechanism involves respiratory centers located in the medulla and pons that control inspiration and expiration. Chemical regulation occurs through central and peripheral chemoreceptors that detect changes in blood oxygen, carbon dioxide, and hydrogen ion levels and stimulate the respiratory centers. Factors like exercise, voluntary control, and lung irritants can also affect respiration.


![• Effect of CO2 on chemosensitive neurons:
→the excitation effects peaks the 1st hours after the
increment in blood [CO2]
→after 2 days the effect is decreased because of:
a)- renal adjustment of [H+].
b)- increased bicarbonate ions that enter the CSF
and bind to H+](https://image.slidesharecdn.com/regulationofrespiration-ap-converted-200729041528/85/Regulation-of-respiration-ap-converted-30-320.jpg)
![Acclimatization
• “Chronic breathing of low O2”
→Mountain climbers ascend slowly over a period of
days→ causing deep breathing and withstanding low
PO2
→ because after 2 days 4/5th of the sensitivity of
receptors to CO2 an H+ is lost
→ slow [O2]→ ↑ventilation by 400% whereas acute
exposure of low [O2] will only ↑ventilation by 70%](https://image.slidesharecdn.com/regulationofrespiration-ap-converted-200729041528/85/Regulation-of-respiration-ap-converted-31-320.jpg)
![Regulation during exercise
• → In exercise O2 consumption and CO2
formation is increased 20x
→ the ventilation is increased so PO2, PCO2 and
pH remain Normal
→ when the brain sends its signals to the
muscles it also send collateral signals to the
brain stem to increase ventilation.
→then chemical factors play a significant role
to maintain [O2],[CO2]](https://image.slidesharecdn.com/regulationofrespiration-ap-converted-200729041528/85/Regulation-of-respiration-ap-converted-32-320.jpg)
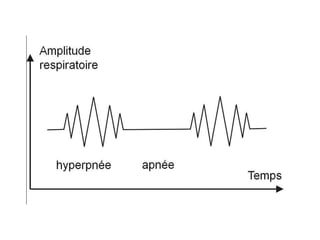
![Periodic “Cheyne-Stokes” breathing
→ person over-breathes→ ↑[O2],↓[CO2]
→after seconds these are sensed by the resp.
centre→ inhibition of excess ventilation→
opposite cycle begins→ ↓[O2],↑[CO2]
→after seconds these are sensed by the resp.
centre→ the person is again over-breathing](https://image.slidesharecdn.com/regulationofrespiration-ap-converted-200729041528/85/Regulation-of-respiration-ap-converted-34-320.jpg)