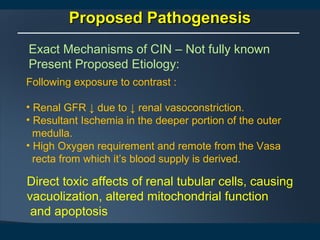
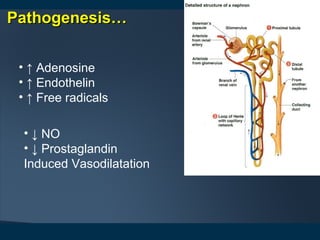
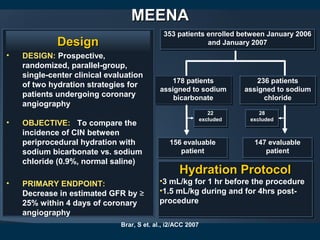
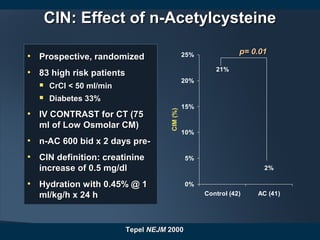
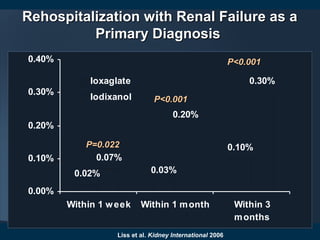
1) Contrast induced nephropathy (CIN) is a serious complication of cardiac procedures and can lead to acute renal failure, increased mortality, and long term renal dysfunction.
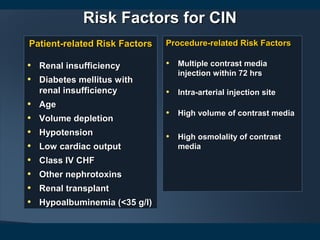
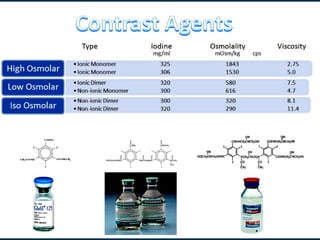
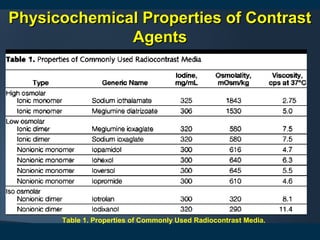
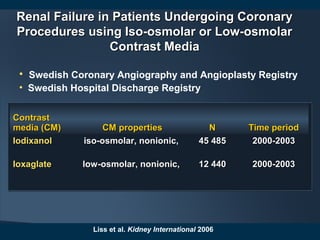
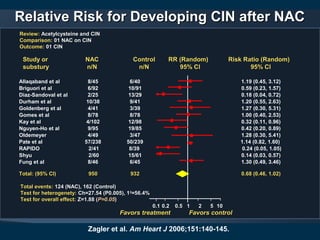
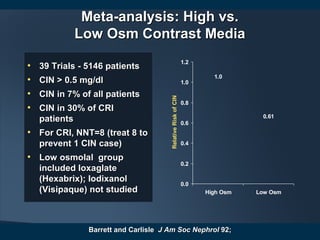
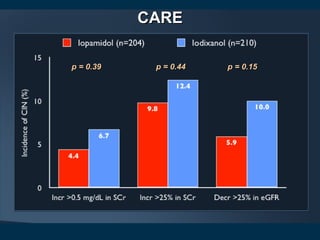
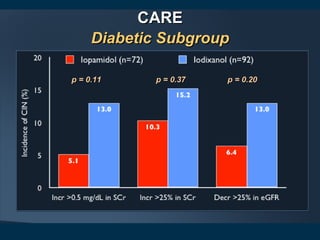
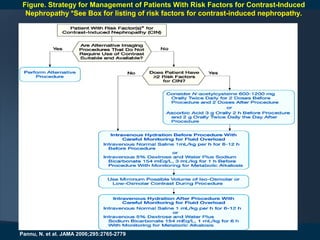
2) Many risk factors increase a patient's likelihood of developing CIN, including pre-existing renal insufficiency, diabetes, older age, hypotension, and the volume and osmolality of contrast agent used.
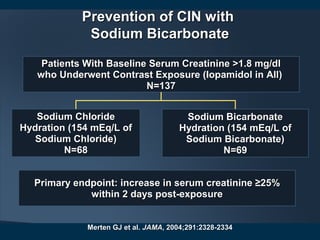
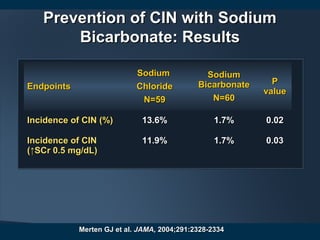
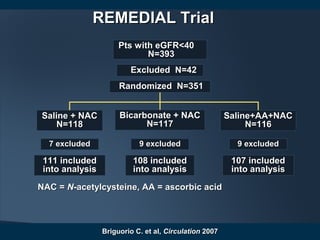
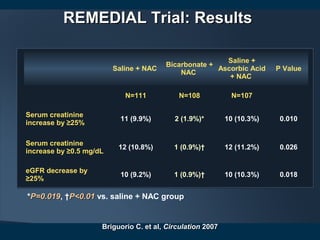
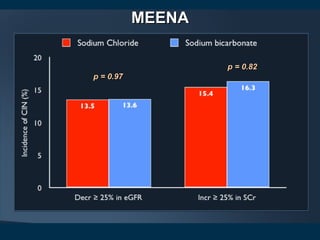
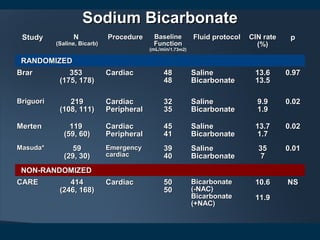
3) Preventive strategies aim to reduce renal ischemia and oxidative stress through hydration with intravenous fluids like sodium bicarbonate or sodium chloride, as well as pharmacological interventions including N-acetylcysteine. Larger clinical trials are still needed to determine the most effective prevention protocols.
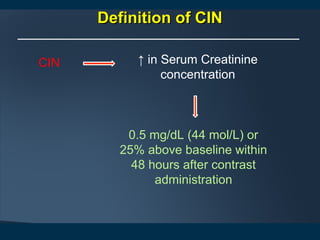
![How to Assess Renal Function?How to Assess Renal Function?
Abbreviated Modification of Diet in Renal Disease
equations (MDRD) equation:
eGFR, ml/min/1.73 m2
= 186 x (Serum Creatinine [mg/dL]) -1.154 x
(Age-0.203x (0.742 if female) x (1.210 if African American)
(140- age) x Body Weight [kg]*
Creatinine Clearance, ml/min =
* Multiple by 0.8 in female
Cockcroft-Gault equation:
Serum Creatinine mg/dL] x 72](https://image.slidesharecdn.com/actualpresentationofcin-130607095025-phpapp01/85/Contrast-Induced-Nephropathy-6-320.jpg)
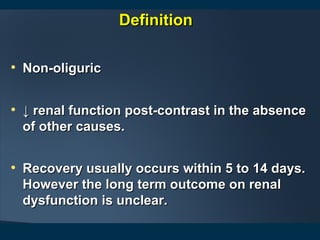


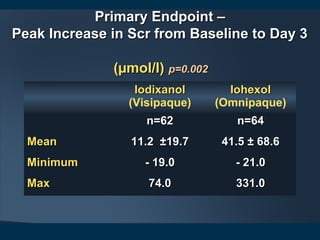
![NEPHRICNEPHRIC Study: ProtocolStudy: Protocol
• Randomized, double blind, prospective, multicenterRandomized, double blind, prospective, multicenter
• Primary endpoint: peak increase in serum creatininePrimary endpoint: peak increase in serum creatinine
concentration @ 3 days after angiographyconcentration @ 3 days after angiography
Patients with diabetes and serum creatinine 1.5-3.5 mg/dl whoPatients with diabetes and serum creatinine 1.5-3.5 mg/dl who
underwent coronary or aortofemoral angiographyunderwent coronary or aortofemoral angiography
Iso-osmolar, non-ionicIso-osmolar, non-ionic
Iodixanol [Visipaque]Iodixanol [Visipaque]
N=64N=64
Mean Contrast Volume = 163 mlMean Contrast Volume = 163 ml
PTCA – 17%PTCA – 17%
Low-osmolar, non-ionicLow-osmolar, non-ionic
Iohexol [Omnipaque]Iohexol [Omnipaque]
N=65N=65
Mean Contrast Volume =Mean Contrast Volume = 162 ml162 ml
PTCA – 25%PTCA – 25%
Aspelin P et al,Aspelin P et al, NEJMNEJM, 2003; 348: 491-499, 2003; 348: 491-499](https://image.slidesharecdn.com/actualpresentationofcin-130607095025-phpapp01/85/Contrast-Induced-Nephropathy-39-320.jpg)


















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















