2
Introduction
Incidence ofCIN in normal renal function even in the presence
of diabetes – 1-2%
In patient with pre existing renal impairment or in presence of
risk factors 25%
It is responsible for 11 % cases of hospital acquired AKI.
Kidney disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO CLINICAL PRACTICAL GUIDELINES FOR ACUTE
KIDNEY INJURY. Kidney Int 2012;Suppl 2:1 -138;
3.
3
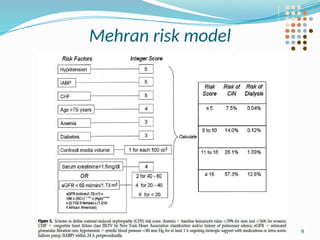
Mehran R, NikolskyE. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl.
2006(100):S11–5.
An absolute
increase in
serum
creatinine of
0.5 mg/dL
≥ or
a 25%
≥
relative
increase in
serum
creatinine
from the
baseline value
At 48–72
hours after
exposure to
contrast
agent, peaks
at 3–5 days
in the
absence of
alternative
causes for
acute
kidney
injury
Definition
4.
4
KDIGO Definition
CI-AKI isdefined by the Kidney Disease Global Outcomes (KDIGO)
guidelines as an “increase in serum creatinine of 0.3 mg/dL or greater within
48 hours of contrast use or a 50% or greater increase from baseline
serum creatinine within 7 days”
• or an increase in cystatin C
>10%
Kidney disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO CLINICAL PRACTICAL GUIDELINES FOR ACUTE
KIDNEY INJURY. Kidney Int 2012;Suppl 2:1 -138;
5.
5
Contrast-associated acute kidneyinjury (CA-AKI): Any AKI occurring
within 48 hours after the administration of contrast media.
Neither term implies a causal relationship between contrast medium
administration and an AKI event.
Contrast-induced acute kidney injury (CI-AKI): CI-AKI is the subset of CA-
AKI that can be causally linked to contrast media administration.
CI-AKI implies a causal relationship between intravenous contrast media
and the development of AKI.
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus
Statements from the
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
11
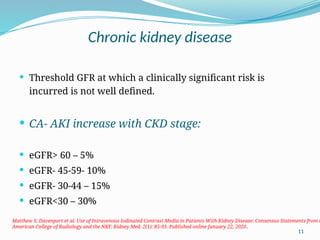
Chronic kidney disease
Threshold GFR at which a clinically significant risk is
incurred is not well defined.
CA- AKI increase with CKD stage:
eGFR> 60 – 5%
eGFR- 45-59- 10%
eGFR- 30-44 – 15%
eGFR<30 – 30%
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus Statements from t
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
12.
12
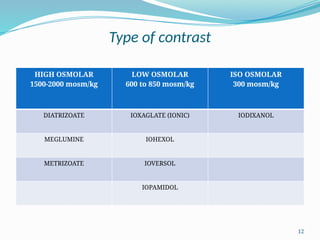
Type of contrast
HIGHOSMOLAR
1500-2000 mosm/kg
LOW OSMOLAR
600 to 850 mosm/kg
ISO OSMOLAR
300 mosm/kg
DIATRIZOATE IOXAGLATE (IONIC) IODIXANOL
MEGLUMINE IOHEXOL
METRIZOATE IOVERSOL
IOPAMIDOL
13.
13
Dose of contrast
Dose < 125 ml – safe but not free of risk.
DM patients with creatinine > 5mg/dl - <20 ml
Dose < 10 ml can be safely used in advanced kidney disease.
V/CrCl ratio above 3.7 independently predicts CI-AKI.
Kian K, Wyatt C et al. Safety of low-dose radiocontrast for interventional AV fistula salvage in stage 4 chronic kidney disease
patients. Kidney Int. 2006 Apr;69(8):1444-9.
14.
14
Type of procedure
Highest risk with interventional procedures than diagnostic.
Intra-arterial administration is associated with higher rate of
CIN and LOCM is more beneficial over HOCM than with
intravenous use.
Cardiac angiography higher risk, intra arterial injection,
increase chances of embolization, contrast medium dose to
kidney will be more abrupt and concentrated.
Kian K, Wyatt C et al. Safety of low-dose radiocontrast for interventional AV fistula salvage in stage 4 chronic kidney disease
patients. Kidney Int. 2006 Apr;69(8):1444-9.
15.
15
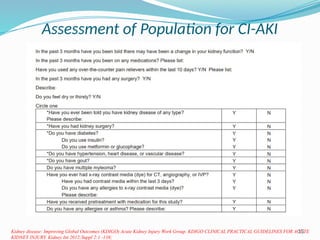
Assessment of Populationfor CI-AKI
Kidney disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO CLINICAL PRACTICAL GUIDELINES FOR ACUTE
KIDNEY INJURY. Kidney Int 2012;Suppl 2:1 -138;
Screening for pre existing renal impairment : SCr
concentration is > 1.3 mg/dl in men and >1.0 mg/dl) in
women, equivalent to an eGFR < 60 ml/min per 1.73 m2.
Choyke questionnaire : reduced the number of patients in
need of a blood sample by 67%.
Negative urine protein test and no history of diseases
potentially associated with renal impairment, none had a
SCr level >2.0 mg/dl, and only 1% had a level >1.7 mg/dl.
16.
16
Assessment of Populationfor CI-AKI
Work Group recommends that, when a recent SCr is not
available, a simple questionnaire or a dipstick testing for
urine protein may be useful for identifying pre-existing
kidney disease
Kidney disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO CLINICAL PRACTICAL GUIDELINES FOR ACUTE
KIDNEY INJURY. Kidney Int 2012;Suppl 2:1 -138;
17.
17
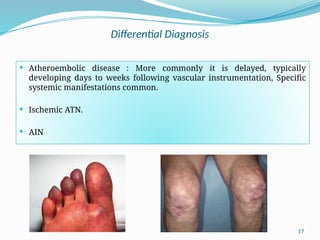
Differential Diagnosis
Atheroembolicdisease : More commonly it is delayed, typically
developing days to weeks following vascular instrumentation, Specific
systemic manifestations common.
Ischemic ATN.
AIN
19
Which patients needprophylaxis??
Indicated : AKI, eGFR <30ml/min/1,73m2, patient not on dialysis,
eGFR- 30-44 + high risk factors
Not indicated – stable GFR, chronic hemodialysis patients,
patients with risk of heart failure.
KDIGO- Recommended for patients not on dialysis with GFR<45
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus Statements from t
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
20.
20
Non Pharmacological Prevention
Use lowest possible dose of contrast.
Use intravenous route of administration than intra-arterial.
KDIGO recommends either iso osmolar or low osmolar contrast
media rather than high osmolar contrast media in patient with
increase risk of CI-AKI.
Remote ischemic preconditioning
22
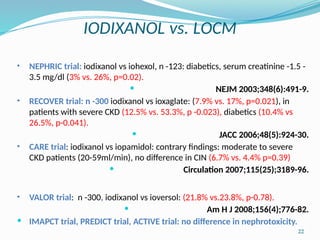
IODIXANOL vs. LOCM
•NEPHRIC trial: iodixanol vs iohexol, n -123: diabetics, serum creatinine -1.5 -
3.5 mg/dl (3% vs. 26%, p=0.02).
NEJM 2003;348(6):491-9.
• RECOVER trial: n -300 iodixanol vs ioxaglate: (7.9% vs. 17%, p=0.021), in
patients with severe CKD (12.5% vs. 53.3%, p -0.023), diabetics (10.4% vs
26.5%, p-0.041).
JACC 2006;48(5):924-30.
• CARE trial: iodixanol vs iopamidol: contrary findings: moderate to severe
CKD patients (20-59ml/min), no difference in CIN (6.7% vs. 4.4% p=0.39)
Circulation 2007;115(25);3189-96.
• VALOR trial: n -300, iodixanol vs ioversol: (21.8% vs.23.8%, p-0.78).
Am H J 2008;156(4);776-82.
IMAPCT trial, PREDICT trial, ACTIVE trial: no difference in nephrotoxicity.
23.
23
Four Principal Strategies
Hydration.
Use of phamocological agents to counteract the nephrotoxic
effect of contrast.
Provision of preemptive RRT to remove contrast from
circulation.
24.
24
Hydration
•Counteract both hemodynamicalterations and direct tubulotoxic effects.
•Suppression of vasopressin, RAS system, increase synthesis of
vasodilatory prostaglandin.
•Decrease cellular damage by dilution of contrast medium
Dose, duration no clear evidence
Protocol: 1 mL/kg/h, 12 h before and 12 h after
procedure or 3 mL/kg/h, 1 h before procedure; and 1
mL/kg/h, 3–6 h after procedure
25.
25
Isotonic vs. HypotonicSaline
Solomon et al. (1994 NEJM) published that 0.45% NS was
more effective in preventing CIN than IV mannitol or
furosemide (11% vs 28% vs 40%)
In a study by Mueller et al, intravenous administration of isotonic
saline was found to be superior, compared with half-isotonic
saline, in reducing the rates of CIN after percutaneous coronary
intervention (0.7% versus 2%, respectively).
27
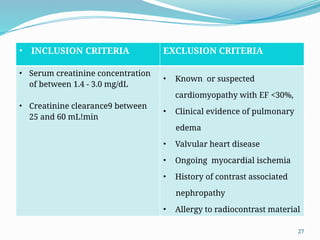
• INCLUSION CRITERIAEXCLUSION CRITERIA
• Serum creatinine concentration
of between 1.4 - 3.0 mg/dL
• Creatinine clearance9 between
25 and 60 mL!min
• Known or suspected
cardiomyopathy with EF <30%,
• Clinical evidence of pulmonary
edema
• Valvular heart disease
• Ongoing myocardial ischemia
• History of contrast associated
nephropathy
• Allergy to radiocontrast material
28.
28
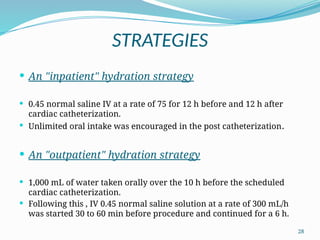
STRATEGIES
An "inpatient"hydration strategy
0.45 normal saline IV at a rate of 75 for 12 h before and 12 h after
cardiac catheterization.
Unlimited oral intake was encouraged in the post catheterization.
An "outpatient" hydration strategy
1,000 mL of water taken orally over the 10 h before the scheduled
cardiac catheterization.
Following this , IV 0.45 normal saline solution at a rate of 300 mL/h
was started 30 to 60 min before procedure and continued for a 6 h.
30
Limitations
Applicable toselected patients (mild to at most moderate renal
dysfunction)
Safety of this protocol unknown
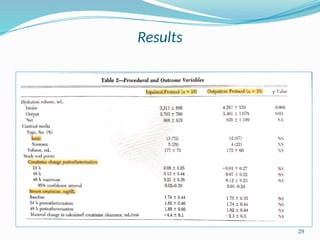
Outpatient hydration strategy in this study resulted in
significantly greater volume administration.
Underpowered study
31.
31
Conclusion
Outpatient hydrationconsists of oral precatheterization and IV
postcatheterization hydration is comparable to 24-h IV hydration for
maintaining a stable serum creatinine for patients with mild-to-moderate
renal dysfunction undergoing elective cardiac catheterization.
32.
32
Oral vs. Intravenoussaline
53 patients were randomly assigned to either unrestricted oral fluids or
to normal saline at 1 mL/kg per hour for 24 hours beginning 12 hours
prior to the scheduled catheterization. AKI was significantly
more common with oral hydration (35 versus 4 %, p-0.005).
33.
33
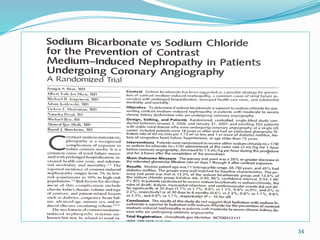
NACL vs. NaHCO3
•10 clinical trials in the past 5 years (largest trial 502 patients).
• 6 had lower incidence of CIN in the NaHCO3 group, 4 showed
no significant benefits
BOSS (Bicarbonate or Saline Study): no difference in the incidence
of CIN in patients with CKD 3,4,5 undergoing CAG.
KDIGO – no recommendation favoring isotonic bicarbonate
or saline.
35
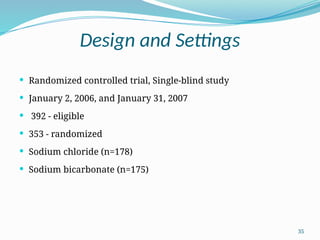
Design and Settings
Randomized controlled trial, Single-blind study
January 2, 2006, and January 31, 2007
392 - eligible
353 - randomized
Sodium chloride (n=178)
Sodium bicarbonate (n=175)
36.
36
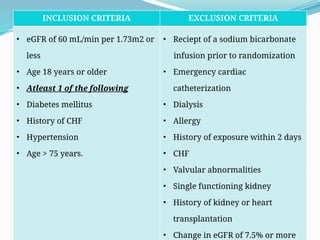
INCLUSION CRITERIA EXCLUSIONCRITERIA
• eGFR of 60 mL/min per 1.73m2 or
less
• Age 18 years or older
• Atleast 1 of the following
• Diabetes mellitus
• History of CHF
• Hypertension
• Age > 75 years.
• Reciept of a sodium bicarbonate
infusion prior to randomization
• Emergency cardiac
catheterization
• Dialysis
• Allergy
• History of exposure within 2 days
• CHF
• Valvular abnormalities
• Single functioning kidney
• History of kidney or heart
transplantation
• Change in eGFR of 7.5% or more
37.
37
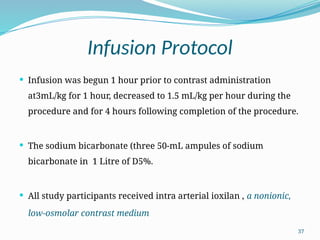
Infusion Protocol
Infusionwas begun 1 hour prior to contrast administration
at3mL/kg for 1 hour, decreased to 1.5 mL/kg per hour during the
procedure and for 4 hours following completion of the procedure.
The sodium bicarbonate (three 50-mL ampules of sodium
bicarbonate in 1 Litre of D5%.
All study participants received intra arterial ioxilan , a nonionic,
low-osmolar contrast medium
38.
38
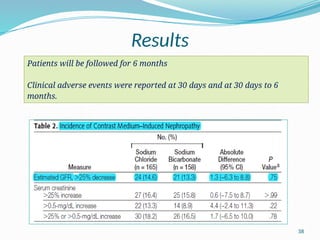
Results
Patients will befollowed for 6 months
Clinical adverse events were reported at 30 days and at 30 days to 6
months.
40
Limitations
The primarystudy end point could not be determined in 11.9%
of the study participants (as serial measurements of serum
creatinine levels were not available)
Physicians performing cardiac catheterization were not blinded
to each patient’s treatment assignment.
Single centered study
41.
41
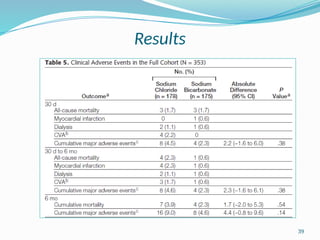
Conclusion
Do notsuggest that hydration with sodium bicarbonate is
superior to sodium chloride hydration in patients with moderate
to severe chronic kidney disease who are undergoing coronary
angiography.
Incidence of CIN didn’t differ by treatment assignment.
Adverse events frequency did not significantly differ between
groups.
42.
42
Hydration
•KDIGO recommends i/vvolume expansion with either sodium
chloride or sodium bicarbonate rather than no i/v volume
expansion , in patients at increased risk for CI-AKI.
43.
43
N acetyl Cysteine
ROS scavenger, decrease depletion of glutathione, increase
production of vasodilatory agents.
There are great heterogeneity and conflicting results in the
available clinical trials and meta analysis examining the
effectiveness of acetyl cysteine in the prevention of contrast
nephropathy.
45
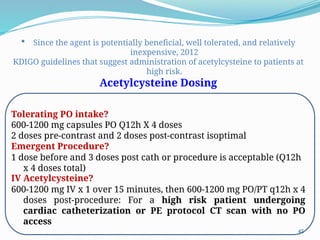
Since theagent is potentially beneficial, well tolerated, and relatively
inexpensive, 2012
KDIGO guidelines that suggest administration of acetylcysteine to patients at
high risk.
Acetylcysteine Dosing
Tolerating PO intake?
600-1200 mg capsules PO Q12h X 4 doses
2 doses pre-contrast and 2 doses post-contrast isoptimal
Emergent Procedure?
1 dose before and 3 doses post cath or procedure is acceptable (Q12h
x 4 doses total)
IV Acetylcysteine?
600-1200 mg IV x 1 over 15 minutes, then 600-1200 mg PO/PT q12h x 4
doses post-procedure: For a high risk patient undergoing
cardiac catheterization or PE protocol CT scan with no PO
access
46.
46
Diuretics
Hypothesis –inhibits active sodium pump decrease
oxygen demand
Anto et al – mannitol beneficial 250 ml 20%/hr with hydration
before and after procedure –(22% CIN in Rx group,70% NS
group)
Solomon et al – exacerbation of CIN on use of furosemide or
mannitol.
Weinstein et al –worsening of renal function
Weisberg et al – no protective effect.
1.Arch Internal Medicine,1981;141:1652-
1656.
2.NEJM,1994;331:1416-1420
3.Nephron 1992;62:413-
415.
47.
47
Calcium channel blockers
Neumayer et al – Nitrendipine. (Beneficial)
Solomon et al – no benefit (78 pts).
Khoury et al – Nifedipine10 mg,administered 1 hr before
imaging made no statistically significant difference in renal
function.
Larsson et al – no benefit of felodipine in diabetics.
Failed to gain as a prophylactic tool to date
48.
48
No Role OfFollowing agents
Statins
Dopamine/Fenoldopam
Theophylline
Prostagladins
Endothelial antagonist
ANP
49.
49
Methods to guidefluid repletion
Left ventricular end-
diastolic pressure
Renal Guard System
Brar SS, Aharonian V, Mansukhani P, et al. Haemodynamic-guided fluid administration for the prevention of contrast- induced
acute kidney injury: the POSEIDON randomised controlled trial. Lancet 2014; 383:1814.
Briguori C, Visconti G, Focaccio A, et al. Renal Insufficiency After Contrast Media Administration Trial II (REMEDIAL II):
RenalGuard System in high-risk patients for contrast-induced acute kidney injury. Circulation 2011; 124:1260.
51
• A randomizedtrial tested the benefit of a fluid
replacement protocol guided by LV end-diastolic pressure
among patients with CKD and other risk factors for CIN.
• In this trial, 396 patients were assigned to LV end-diastolic
pressure-guided fluid management or to a control group.
• All patients received intravenous isotonic saline 3 mL/kg
for one hour prior to cardiac catheterization. LV
end-diastolic pressure was determined in all patients
prior to administration of contrast.
52.
52
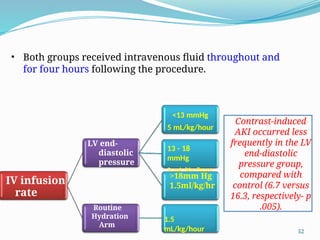
• Both groupsreceived intravenous fluid throughout and
for four hours following the procedure.
IV infusion
rate
LV end-
diastolic
pressure
<13 mmHg
5 mL/kg/hour
13 - 18
mmHg
3 mL/Kg/hour
>18 mmHg
1.5 mL/Kg/hour
Routine
Hydration
Arm
>18mm Hg
1.5ml/kg/hr
1.5
mL/kg/hour
Contrast-induced
AKI occurred less
frequently in the LV
end-diastolic
pressure group,
compared with
control (6.7 versus
16.3, respectively- p
.005).
56
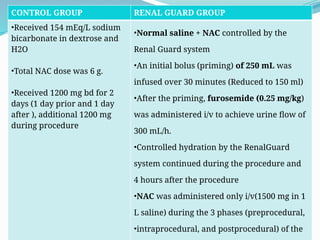
CONTROL GROUP RENALGUARD GROUP
•Received 154 mEq/L sodium
bicarbonate in dextrose and
H2O
•Total NAC dose was 6 g.
•Received 1200 mg bd for 2
days (1 day prior and 1 day
after ), additional 1200 mg
during procedure
•Normal saline + NAC controlled by the
Renal Guard system
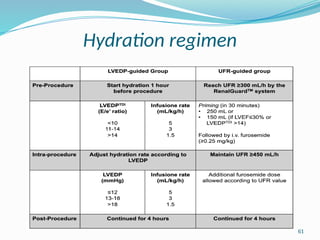
•An initial bolus (priming) of 250 mL was
infused over 30 minutes (Reduced to 150 ml)
•After the priming, furosemide (0.25 mg/kg)
was administered i/v to achieve urine flow of
300 mL/h.
•Controlled hydration by the RenalGuard
system continued during the procedure and
4 hours after the procedure
•NAC was administered only i/v(1500 mg in 1
L saline) during the 3 phases (preprocedural,
•intraprocedural, and postprocedural) of the
57.
57
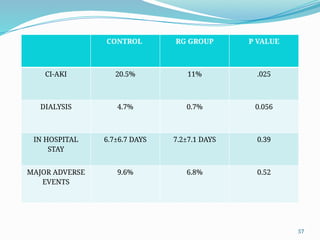
Results
CONTROL RG GROUPP VALUE
CI-AKI 20.5% 11% .025
DIALYSIS 4.7% 0.7% 0.056
IN HOSPITAL
STAY
6.7±6.7 DAYS 7.2±7.1 DAYS 0.39
MAJOR ADVERSE
EVENTS
9.6% 6.8% 0.52
58.
58
Limitations
Open labelstudy.
Powered on CI AKI (increase creatinine >0.3 mg/dl) but not on hard
clinical end points (dialysis/death).
Larger NAC exposure in control might provide advantage.
NAC was administrated orally in control and i/v in RGG.
59.
59
Conclusion
Renal Guardtherapy, (normal saline + high doses of NAC +
limited (0.25mg/kg) dose of furosemide, seems to be an
effective renoprotective strategy for patients at high risk for CI
AKI.
MYTHOS trial support the effectiveness of renal guard system
in patients with less severe CKD (eGFR<60ml/min/1.73m2)
CI-AKI in renal guard group 5% as compared to standard
hydration 16%
60.
60
REMEDIAL III
RENAL InsufficiencyFollowing Contrast
MEDIA Administration III TriaL
Urine flow rate-guided versus left-ventricular end diastolic pressure-
guided hydration in high-risk patients for contrast-induced acute
kidney injury.
• Multicenter, randomized, single-blind, comparing 2 tailored-hydration
regimens
In all cases iobitridol a low-osmolar, non-ionic contrast agent) was
administered.
Between July 15, 2015 and June 6, 2019, N-708
62
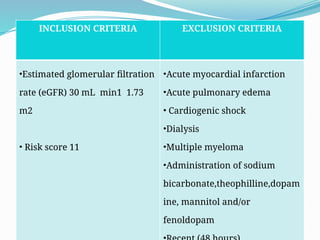
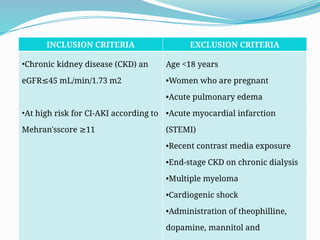
INCLUSION CRITERIA EXCLUSIONCRITERIA
•Chronic kidney disease (CKD) an
eGFR 45 mL/min/1.73 m2
≤
•At high risk for CI-AKI according to
Mehran'sscore 11
≥
Age <18 years
•Women who are pregnant
•Acute pulmonary edema
•Acute myocardial infarction
(STEMI)
•Recent contrast media exposure
•End-stage CKD on chronic dialysis
•Multiple myeloma
•Cardiogenic shock
•Administration of theophilline,
dopamine, mannitol and
63.
63
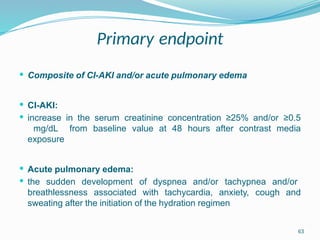
Primary endpoint
Compositeof CI-AKI and/or acute pulmonary edema
CI-AKI:
increase in the serum creatinine concentration ≥25% and/or ≥0.5
mg/dL from baseline value at 48 hours after contrast media
exposure
Acute pulmonary edema:
the sudden development of dyspnea and/or tachypnea and/or
breathlessness associated with tachycardia, anxiety, cough and
sweating after the initiation of the hydration regimen
64.
64
Results
Primary endpoint, CI AKI for UFR guided vs LVEDP
guided angiography was 5.7% vs 10.3% (p- 0.036)
UFR-guided approach (carried out by the RenalGuard system) is
superior to the LVEDP-guided hydration regimen to prevent the
composite of CI-AKI and/or acute pulmonary edema in high-risk patients.
67
Role Of RRT
Small size
Lack of protein binding
Small volume of distribution
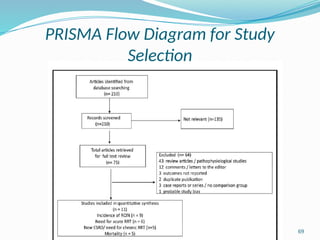
STUDIES ELIGIBLE FOR THIS ANALYSIS
Studies which compare peri procedural RRT with standard
medical treatment
Studies which contained atleast > 10 patients
68.
68
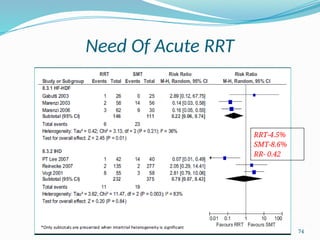
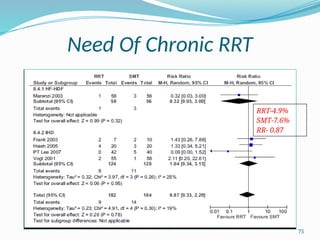
OUTCOMES
PRIMARY OUTCOME SECONDARYOUTCOME
Increase in creatinine > 0.5mg/dl Need of temporary acute RRT
Need of permanent RRT
Long term changes in renal
functions
Death
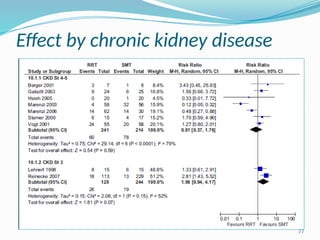
78
Discussion
Significant heterogeneity
HD- increase risk of RCIN
HDF/HF- not affect occurrence of RCIN
Result of RRT related toxicity, hypoperperfusion occur 20 min
after contrast administration.
79.
79
Conclusion
Use ofcreatinine based definition of RCIN.
No clear benefit of RRT in stage 4-5
RRT ineffective or even harmful in stage 3
Insufficient evidence to support RRT for prevention
of RCIN
Limitations
81
Stage 4-5 withoutdialysis patients
Potential risk of AKI
Relative contraindication
For life threatening diagnosis, it should not be withheld.
Neither acute nor CRRT should be initiated.
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus Statements from t
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
82.
82
Patients with SingleKidney
Patients with single normal or partially functioning kidney (kidney
agenesis, nephrectomy, transplant) should be managed similarly to
patients with two normal kidneys.
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus Statements from t
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
Infants and Children
Aforementioned recommendations should not be altered for infants and
children
Minimal data assessing risk of CI-AKI in this population.
Recommendations for this population are largely based on extrapolated
adult data.
83.
83
Withholding other medications??
Patients with AKI and eGFR< 30 withhold non essential
medications 48 hour before and after exposure.
With hold RAAS –controversial, lack of evidence
Metformin should be withheld (eGFR<30, eGFR-30-59 decision
to stop should be individualized by clinicians)
Matthew S. Davenport et al. Use of Intravenous Iodinated Contrast Media in Patients With Kidney Disease: Consensus Statements from t
American College of Radiology and the NKF. Kidney Med. 2(1): 85-93. Published online January 22, 2020.
84.
84
Summary
True riskof CI-AKI remains unknown.
Prophylaxis patients without contraindication (eg, heart failure) who have
acute kidney injury (AKI) or an estimated glomerular filtration rate (eGFR) less
than 30 mL/min/1.73 m2 who are not undergoing maintenance dialysis.
May be considered in individual high-risk circumstances with an eGFR of 30–44
mL/min/1.73 m2.
Solitary kidney should not independently influence decision.
Lowering of contrast media dose below a known diagnostic threshold should be
avoided .
Nephrotoxic medications should be withheld by the referring clinician in patients
at high risk.
Renal replacement therapy should not be initiated or altered solely based on
contrast media administration.
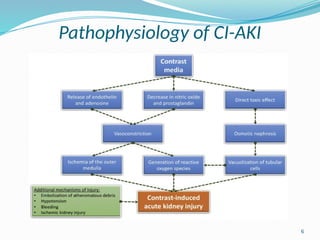
#6 Increase viscosity of tubular fluid , ppt of contrast with urinary protein increase exposure of tubules to conrast medium
#13 DM patients with creatinine > 5mg/dl risk from as little as 20 to 30 ml of contrast
#15 A CI-AKI Consensus Working Panel410 agreed that the risk of CI-AKI becomes clinically important when the baseline
#17 distinguishing between these two forms of
AKI may be dif cult in hemodynamically unstable patients
(“blue toe” syndrome) and livedo reticularis, and laboratory abnormalities that include eosinophilia, eosinophiluria, and hypocomplementemia.
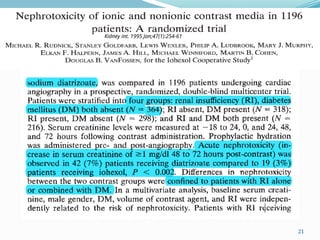
#21 In conclusion, in patients undergoing cardiac angiography, only those with pre-existing RI alone or combined with DM are at higher risk for acute contrast nephrotoxicity. The incidence of acute nephrotoxicity in these high-risk patients is significantly less with the nonionic contrast media iohexol compared to the ionic contrast agent diatrizoate.
#22 Nephric Other end points were an increase in the creatinine concentration of 0.5 mg per deciliter or more, an increase of 1.0 mg per deciliter or more, and a change in the creatinine concentration from day 0 to day 7.
#28 Following completion of the IV hydration period, all treatment with IV fluids was discontinued
#34 Generation of ROS augmented in acidic ph, NAHCO3 stronger impact in lowering intratubular viscosity than isotonic saline
#38 baseline rate obtained prior to the procedure and lowest rate postprocedure on days 1 through 4
#56 This RenalGuard system includes a
closed-loop fluid management system, a high-volume fluid pump, ahigh-accuracy dual weight measuring system, motion-detection artifact
reduction, a single-use intravenous set and urine collection
system that interfaces with a standard Foley catheter, real-time
display of urine and replacement fluid volume, timely alerts to drain
the urine bag or to replace the hydration fluid bag, and safety features
such as automatic air and occlusion detection.
#57 Increase in sCr concentration 0.3 mg/dL above the baseline value at 48 hours after administration of CM
Total volume of hydration was higher in renal guard as compared to other group (2999 vs. 1438)
Furosemide dose to reach the target urine flow was 14±8 mg.
Target urine flow was reached in the 93% of patients.
Additional doses of furosemide (25±35 mg) in 42.5% of patients.
The length of RenalGuard therapy was on average 5 hours 75 minutes
Total volume of hydration was higher in renal guard as compared to other group (2999 vs. 1438)
Furosemide dose to reach the target urine flow was 14±8 mg.
Target urine flow was reached in the 93% of patients.
Additional doses of furosemide (25±35 mg) in 42.5% of patients.
The length of RenalGuard therapy was on average 5 hours 75 minutes
#67 Not because of the contrast removal, its due to bicarbonate based hydration to high risk pts in which we cant give fluid at higher rate to avoid overhydration
Hypothesis ?? Increase effective corculatory volume unlikely with completely isovolemic protocol, recent data raised doubts abiut renoprotective benefits
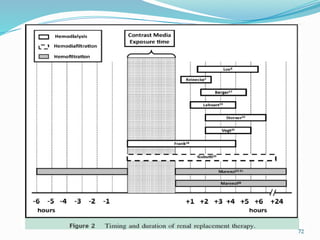
#70 A total of 1010 patients treated in 5 countries are represented in this analysis: 445 patients in the RRT group and 565 in SMT, delay time from contrast exposure to the beginning of HD, when reported, ranged from 20-280 minutes.