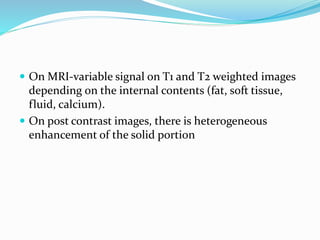
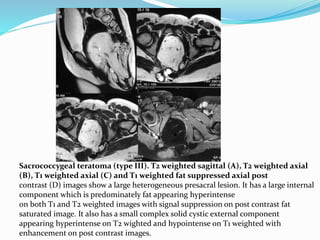
This document discusses spinal dysraphism, which refers to congenital malformations of the spine and spinal cord resulting from incomplete closure of tissues during embryonic development. It describes the normal embryological development of the spinal cord and the various types of spinal dysraphism, including open dysraphisms like myelomeningocele and closed dysraphisms with and without subcutaneous masses. Specific conditions are defined, like lipomyelomeningocele versus lipomyelocele, and imaging features of each type of dysraphism are provided with examples. Chiari malformations that can be associated with open dysraphisms are also reviewed.



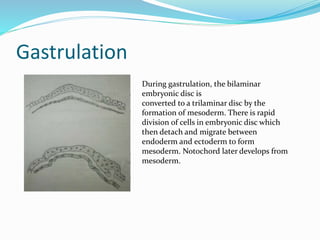
![ EMBRYOLOGY: Development of spinal cord occurs
during early embryogenesis (between 2-6 wk of
gestation]
stages - gastrulation, primary neurulation and
secondary neurulation](https://image.slidesharecdn.com/spinaldysraphism-181213181830/85/Spinal-dysraphism-9-320.jpg)
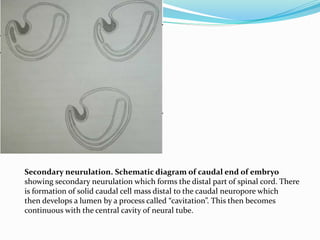
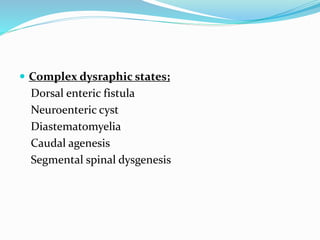
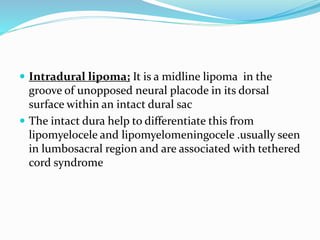
![Primary neurulation
Primary neurulation. A: Thickening of embryonic
ectoderm is seen
dorsal to notochord to form neuroectoderm and neural
plate; B: Neural plate
invaginates along its central axis to form neural groove.
Neural folds are formed
on both sides of the neural groove; C: The neural plate then
bends and neural
folds fuse together to form neural tube and simultaneously
separate from
surface ectoderm (dysjunction]](https://image.slidesharecdn.com/spinaldysraphism-181213181830/85/Spinal-dysraphism-11-320.jpg)
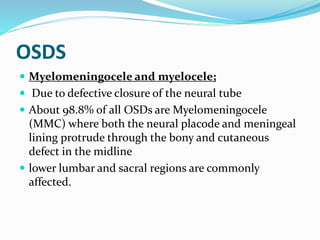
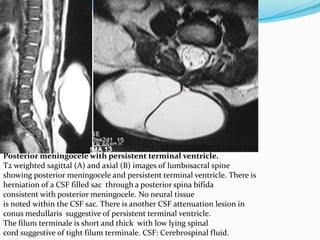
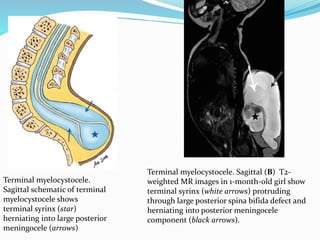
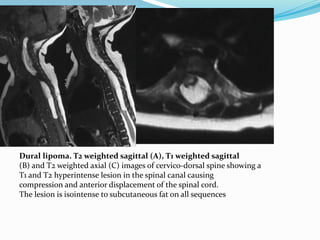
![Terminal myelocystocele
Herniation of a dilated terminal central canal forming
terminal syringohydromyelia (syringocele) through a
posterior vertebral defect into an expanded CSF filled
dural sheath (meningocele]
The inner terminal syrinx communicates with the
central canal of the spinal cord and the outer
meningocele is continuous with the spinal
subarachnoid space. The syringocele and meningocele
usually do not communicate with each other](https://image.slidesharecdn.com/spinaldysraphism-181213181830/85/Spinal-dysraphism-41-320.jpg)
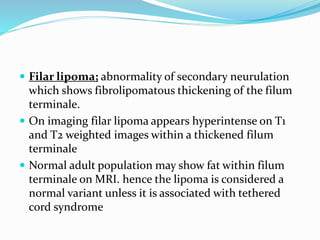
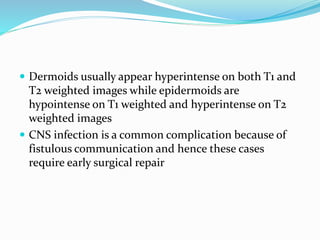
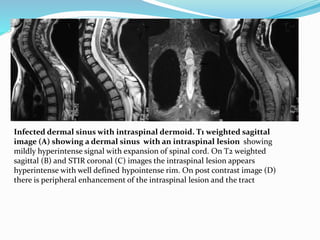
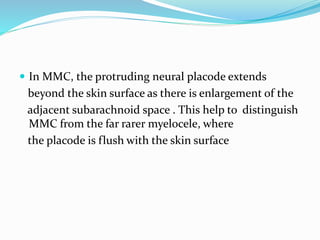
![Dermal sinus. Sagittal schematic (A) and sagittal T2-weighted MR image (B) in 9-year-
old girl show intradural dermoid (stars) with tract extending from central canal to skin
surface (black arrows). Note tenting of dural sac at origin of dermal sinus (white
arrows]](https://image.slidesharecdn.com/spinaldysraphism-181213181830/85/Spinal-dysraphism-54-320.jpg)