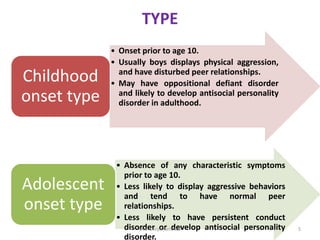
The document discusses conduct disorder, which affects 1-4% of children and is characterized by antisocial behavior that impairs functioning. It defines conduct disorder as a repetitive pattern of violating others' rights or social norms. Causes include biological and psychosocial factors like genetics, family environment, and peer associations. Diagnosis requires at least 3 behaviors like aggression, property destruction, deceit, or rule violations in the past year. Treatments include family therapy, social skills training, cognitive behavioral therapy, and sometimes medication. Schools can provide specialized programming, parent training, and social emotional learning.