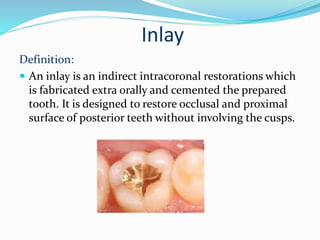
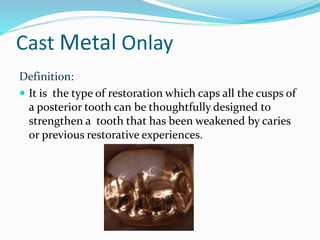
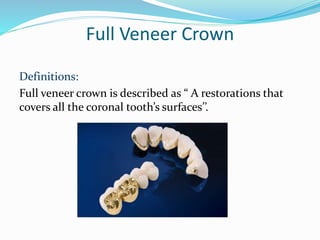
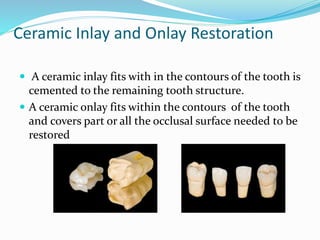
The document discusses various types of complex dental restorations including cast metal restorations, tooth-colored restorations, and CAD-CAM based restorations. It provides details on materials, indications, contraindications, advantages and disadvantages, and fabrication procedures for cast metal inlays, onlays, partial veneer crowns, full veneer crowns, indirect composite inlays/onlays, ceramic inlays/onlays, and CAD-CAM based restorations. It also covers pin-retained restorations and inlay-retained bridges.