Downloaded 18 times






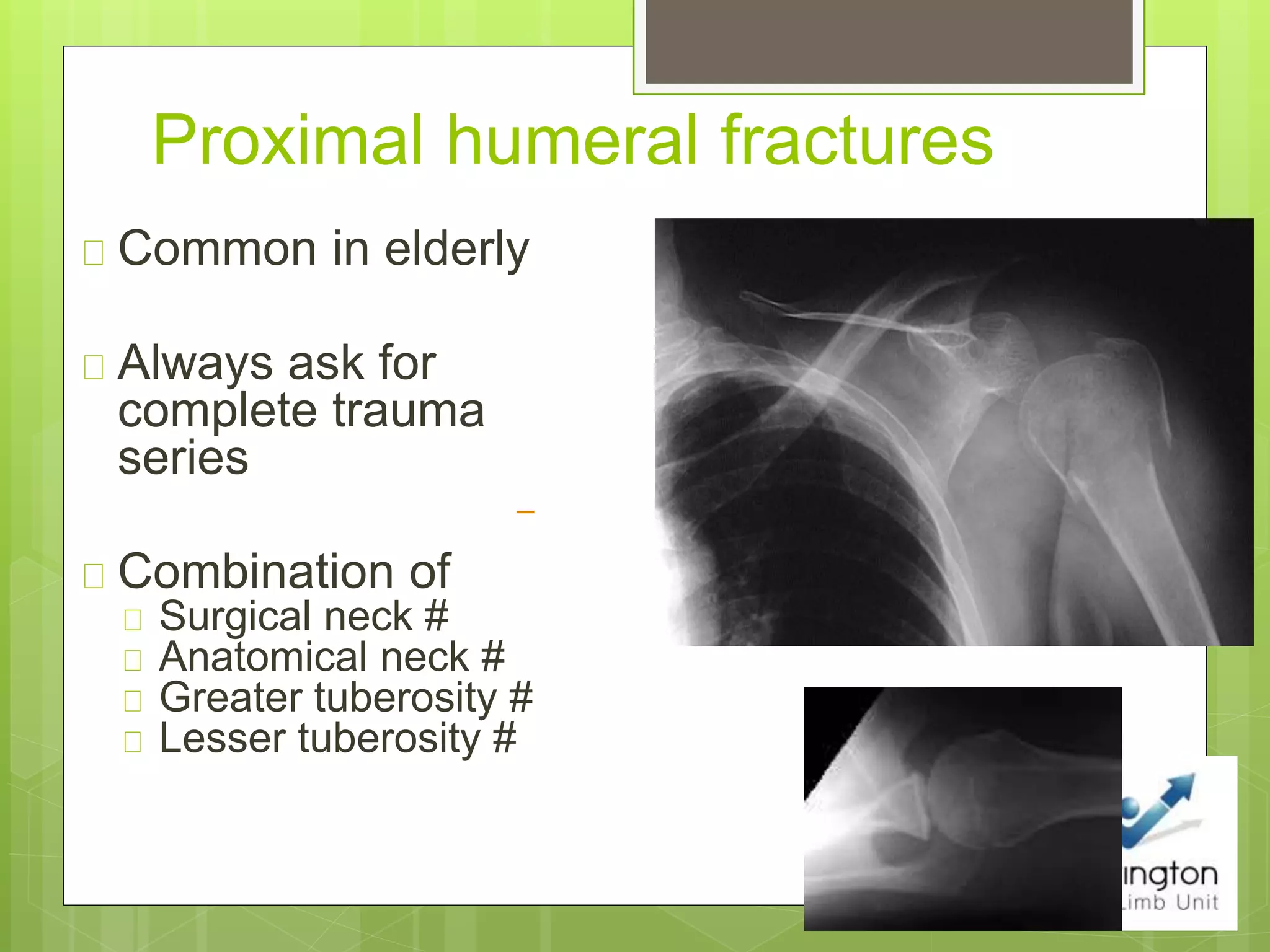
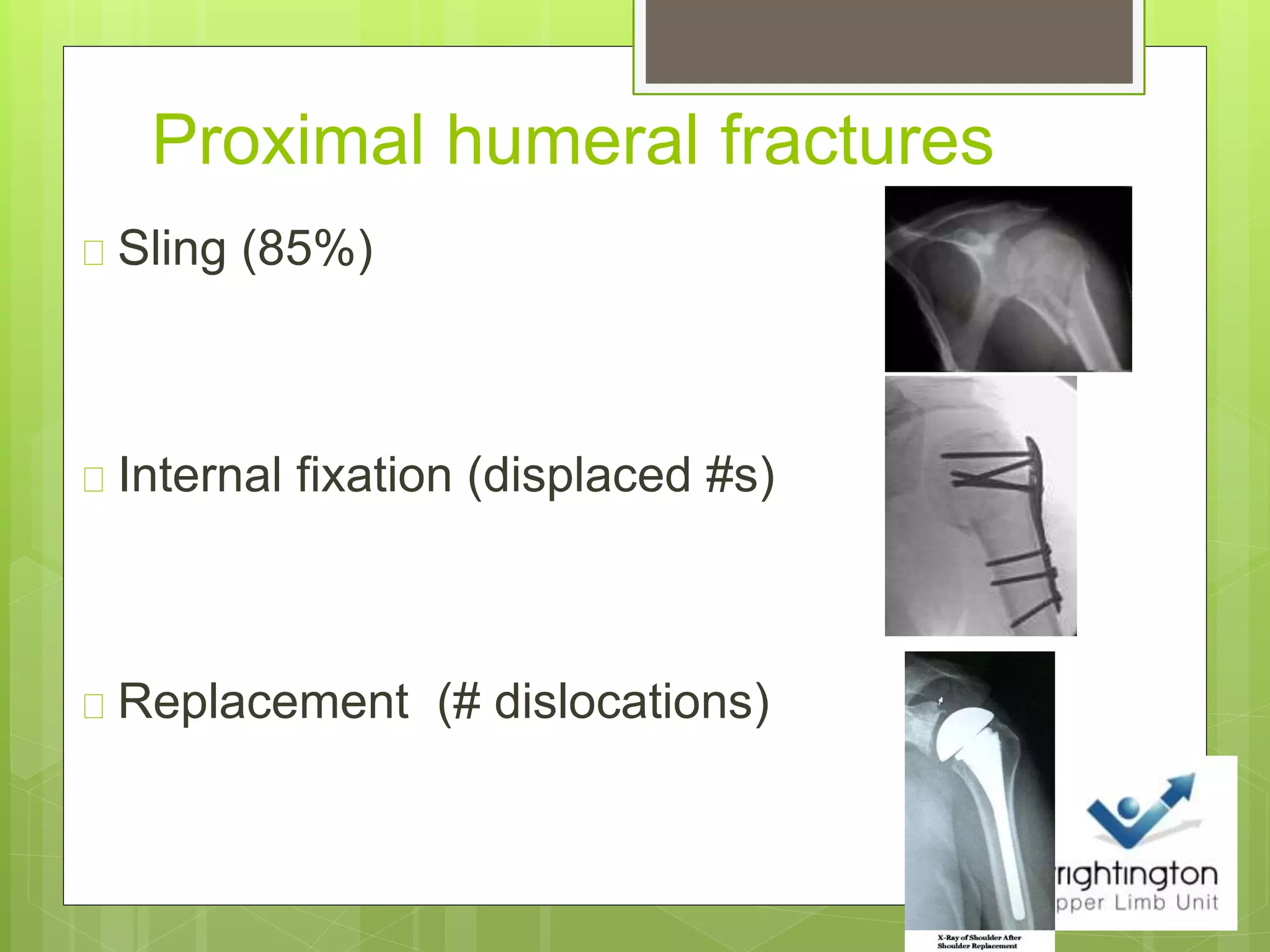


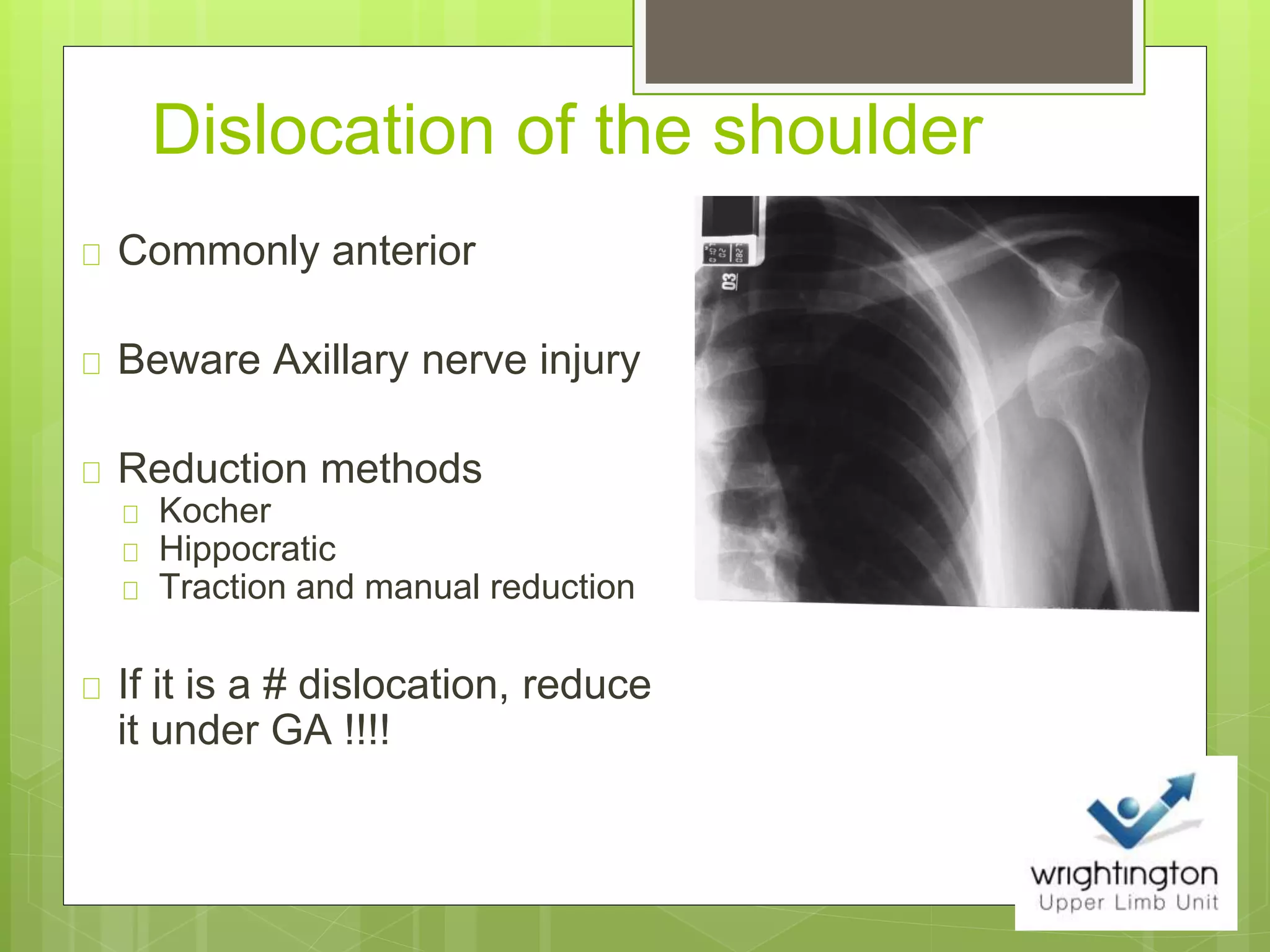






The document discusses common shoulder fractures including clavicle fractures, proximal humeral fractures, shoulder dislocations, and humeral shaft fractures. Clavicle fractures most often occur in the lateral third and are usually treated conservatively with a sling. Proximal humeral fractures are common in the elderly and often involve the surgical neck. They are typically treated with a sling or internal fixation depending on the degree of displacement. Shoulder dislocations are usually anterior and require reduction, which may need to be done under anesthesia if there is a fracture. Humeral shaft fractures have varying displacement depending on the fracture level and are commonly treated conservatively with a sling or brace, but surgery is indicated for more complex cases. Early mobil























































































