


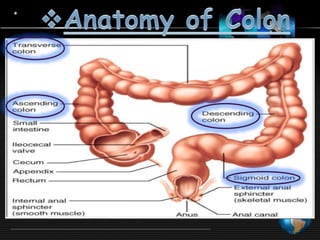
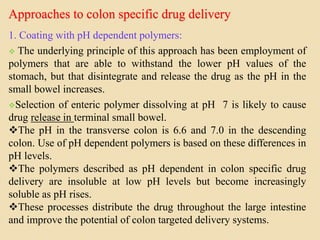

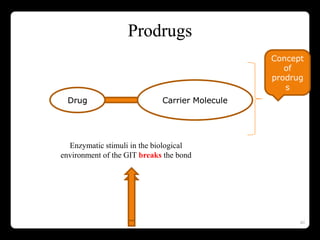
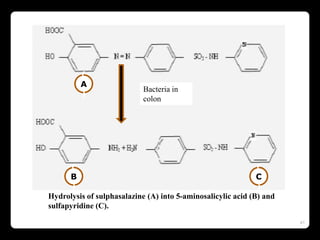


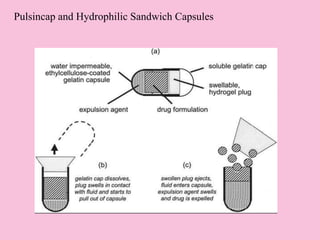
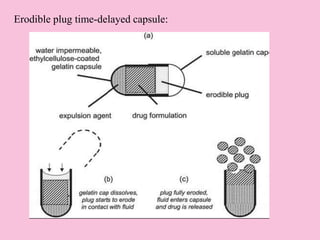
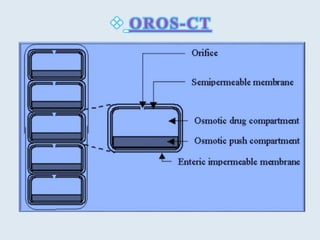
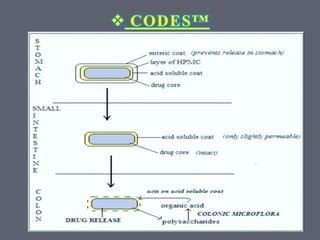
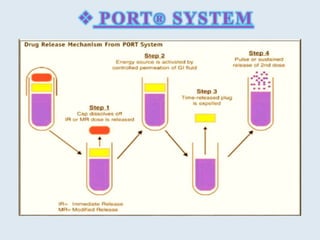
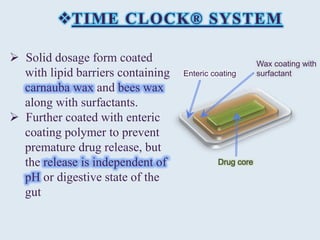
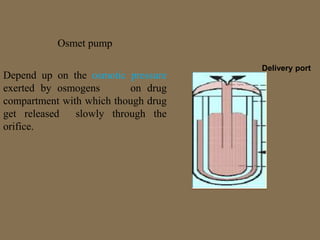
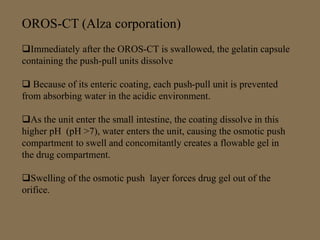
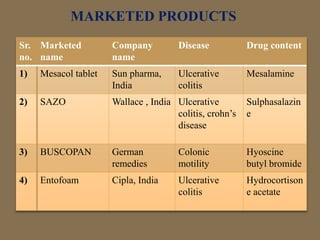
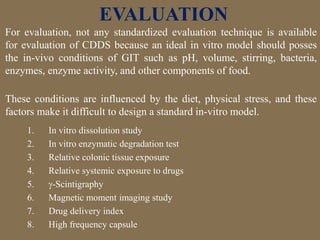


This document discusses targeted drug delivery to the colon. It begins with an introduction to colon targeted drug delivery and describes the anatomy and physiology of the colon. Key criteria for drug selection include drugs used to treat gastrointestinal diseases, those poorly absorbed in the upper GI tract, and drugs that degrade in the stomach and small intestine. Approaches for colon targeting include pH sensitive systems, microbially triggered systems using prodrugs and polysaccharides, timed release systems, and osmotically controlled drug delivery systems. The colon offers advantages for drug delivery including treatment of colonic diseases and absorption of proteins and peptides.




























































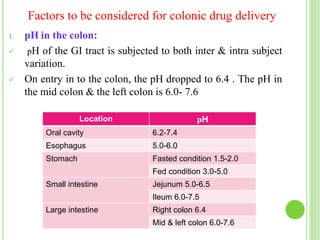
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



