Downloaded 49 times


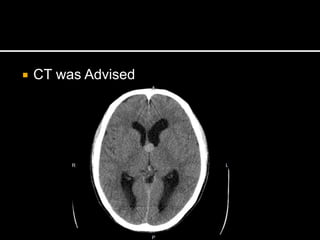
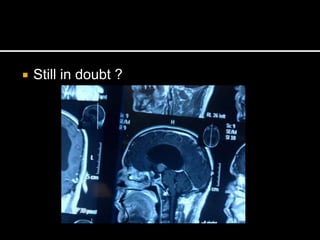


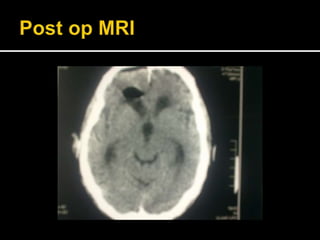
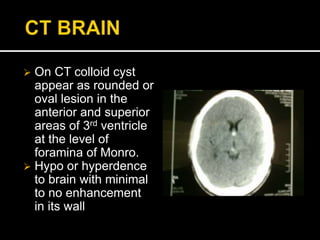
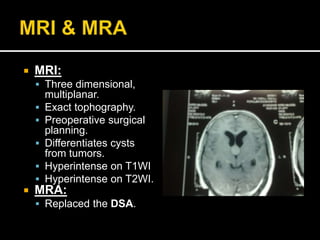

This document discusses a 47-year-old male patient who presented with intermittent headaches and impaired recent memory over the past 3 months. CT scanning revealed a colloid cyst in the anterior third ventricle. The patient underwent an endoscopic resection of the colloid cyst. Post-operatively, the patient's neurological condition was good and his memory disorder had resolved by the 3-month follow up appointment.















































































