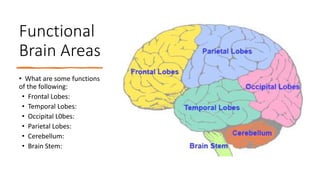
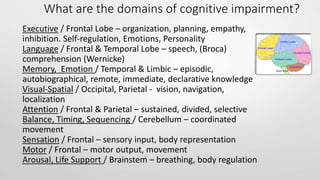
This document provides information on working with individuals with cognitive impairments and dementia. It discusses common symptoms and causes of cognitive impairment, types of dementia and their progression, domains of cognitive function associated with different brain areas, common behaviors seen in dementia, and tips for managing individuals with cognitive impairments or dementias. The document aims to increase understanding of cognitive impairments and dementia in order to better support affected individuals.












































![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)




















