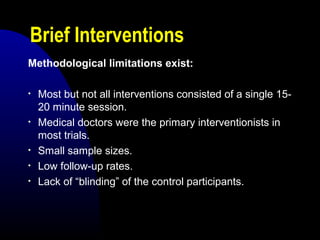
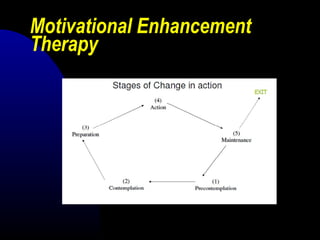
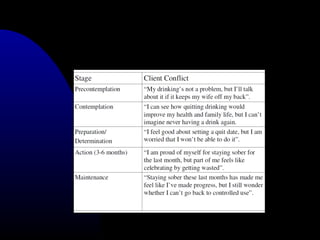
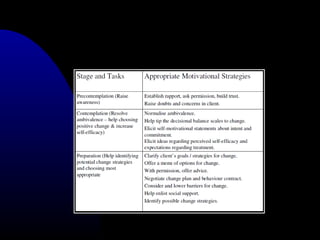
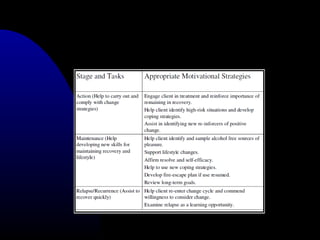
Brief interventions involve short counseling sessions that provide feedback, advice, and support to motivate individuals to reduce risky drinking behaviors. MET is a client-centered counseling style based on motivational interviewing that aims to resolve ambivalence and increase intrinsic motivation for change. Both approaches are time-limited and focus on negotiating drinking reduction rather than requiring abstinence. Screening tools are used to identify hazardous drinkers who could benefit, with brief structured advice or extended brief counseling sessions depending on severity. Motivational strategies like FRAMES are employed to enhance engagement in the process of behavior change.