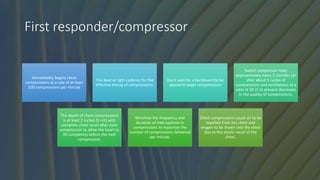
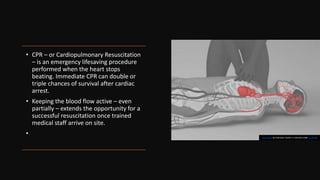
1. CPR is performed when a patient's heart stops beating to maintain blood flow until medical help arrives. It involves chest compressions and ventilations.
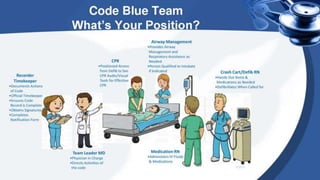
2. During a code blue, nurses play important roles such as performing chest compressions, operating emergency equipment, managing the airway, defibrillating, documenting, and leading the resuscitation efforts.
3. Effective CPR involves high-quality chest compressions, use of an AED/defibrillator, bag-mask ventilation, and coordination among the code blue team to maximize the patient's chances of survival.


![How is CPR Performed?
• There are two commonly known versions of CPR:
• For healthcare providers and those trained: conventional CPR using chest
compressions and mouth-to-mouth breathing at a ratio of 30:2 compressions-
to-breaths. In adult victims of cardiac arrest, it is reasonable for rescuers to
perform chest compressions at a rate of 100 to 120/min and to a depth of at
least 2 inches (5 cm) for an average adult, while avoiding excessive chest
compression depths (greater than 2.4 inches [6 cm]).
• For the general public or bystanders who witness an adult suddenly
collapse: compression-only CPR, or Hands-Only CPR. Hands-Only CPR is CPR
without mouth-to-mouth breaths. It is recommended for use by people who
see a teen or adult suddenly collapse in an out-of-hospital setting (such as at
home, at work, or in a park).](https://image.slidesharecdn.com/cpr-traumafasha-230529175716-cfac7df4/85/Code-blue-Nurses-Role-pptx-6-320.jpg)