Downloaded 1,243 times



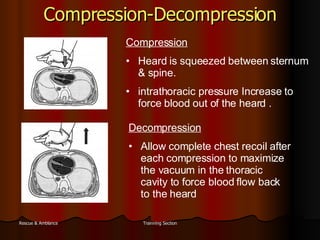









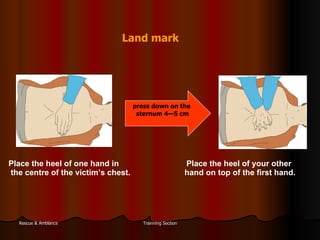



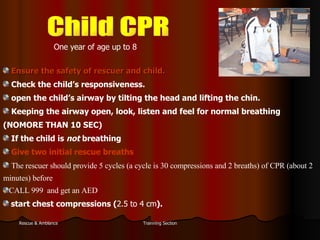
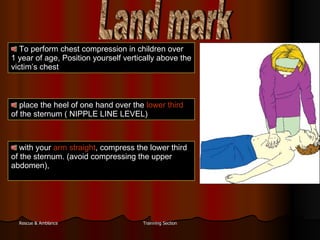










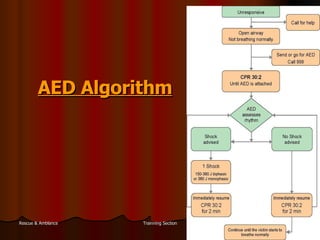


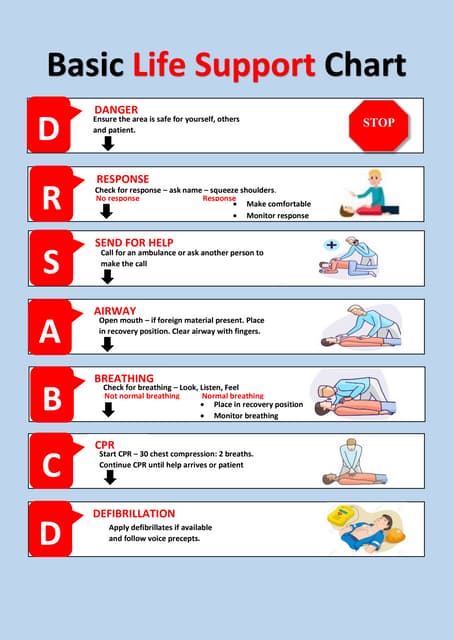
The document summarizes new international guidelines on cardiopulmonary resuscitation (CPR) from 2005. It discusses the importance of early CPR, the proper techniques for CPR including chest compressions and ventilations. It provides guidance on CPR protocols for adults, children, and infants. It also outlines the role of defibrillators in reviving someone in ventricular fibrillation and the proper use of automated external defibrillators.