Downloaded 197 times













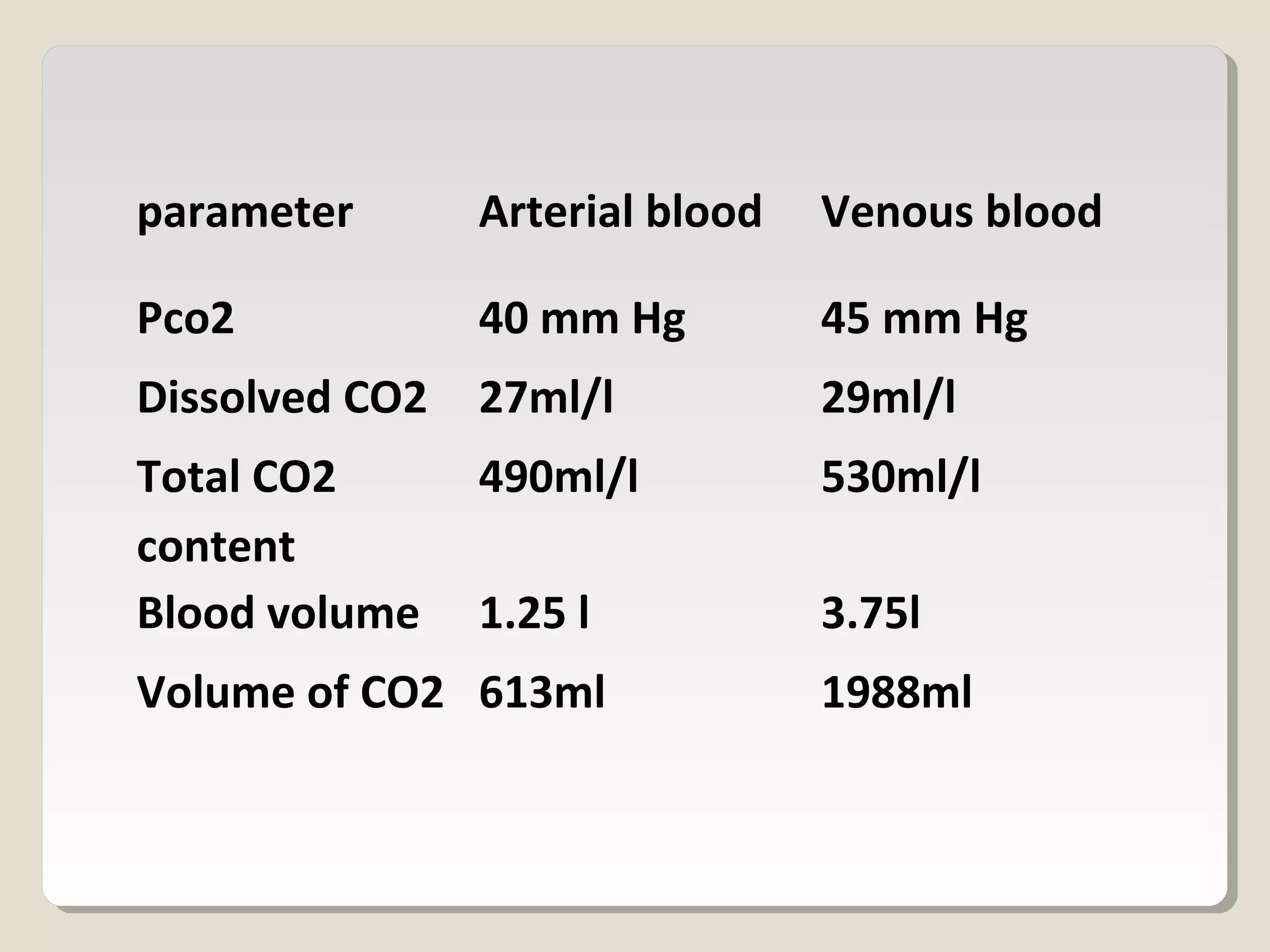









CO2 is transported in the blood in four ways: dissolved, as carbonic acid, as bicarbonates, and as carbamino compounds. CO2 is produced during aerobic metabolism and must be transported to the lungs to be eliminated. It diffuses from tissues into blood and from blood into the alveoli due to partial pressure gradients. In the blood, CO2 is carried as bicarbonates through a chloride shift that maintains electrolyte balance. The CO2 dissociation curve shows the relationship between CO2 levels in blood and partial pressure of CO2. Haldane effect causes more CO2 to be released from blood into alveoli in the presence of oxygen. Hypercapnia occurs when arterial CO






















































































