Downloaded 23 times


![Determination of RV and FRC
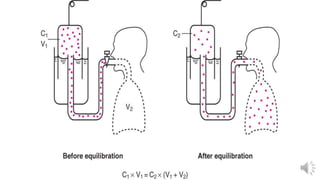
• Helium dilution
• Spirometer of known volume (Vs)and
He Conc.(C1) connected to the patient.
• At end of normal expiration.
-Closed circuit
- After several minutes of breathing.
• C1XV1=C2X(Vs+VL)
• C2= final He conc,VL=FRC.
• [He] initial · Vs = [He] final · (Vs + VL)
• Unknown lung volume can be calculated
At beginning After several minutes](https://image.slidesharecdn.com/lungvolandcapacity-200609063314/85/Lung-volume-and-capacity-18-320.jpg)
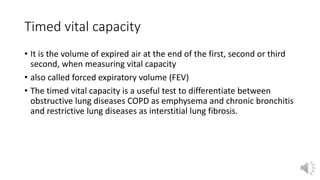
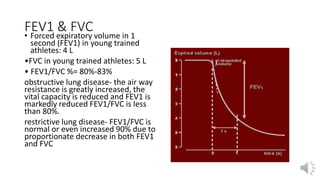
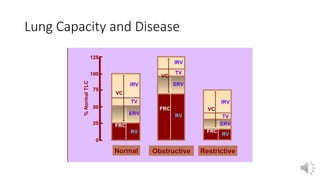

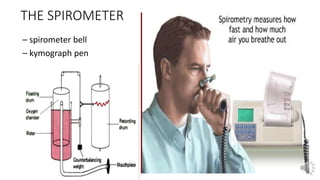
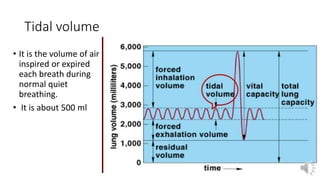
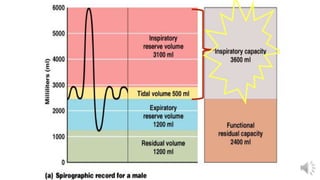
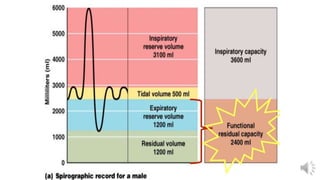
This document discusses lung volumes and capacities and how they are measured. It defines various lung volumes like tidal volume, inspiratory reserve volume, expiratory reserve volume, residual volume, and vital capacity. Lung capacities add together different volumes and include inspiratory capacity, functional residual capacity, and total lung capacity. Lung volumes and capacities can be directly measured using a spirometer or indirectly using helium dilution methods. Abnormal lung volumes and capacities can indicate restrictive or obstructive lung diseases.























































































