Downloaded 35 times
![Radiology for Radiation Oncologist
Radiology of Brain & Spine
Dr Kanhu Charan Patro
MD,DNB[RADIATION ONCOLOGY],MBA,CEPC,PDCR
HOD, Radiation Oncology
MGCHRI, Visakhapatnam, INDIA
M +91 9160470564, drkcpatro@gmail.com 1](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-1-320.jpg)
![Radiology for Radiation Oncologist
Radiology of Brain & Spine
Dr Kanhu Charan Patro
MD,DNB[RADIATION ONCOLOGY],MBA,CEPC,PDCR
HOD, Radiation Oncology
MGCHRI, Visakhapatnam, INDIA
M +91 9160470564, drkcpatro@gmail.com 1](https://image.slidesharecdn.com/cnsradiology-200702165023/75/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-1-2048.jpg)

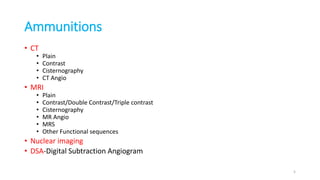

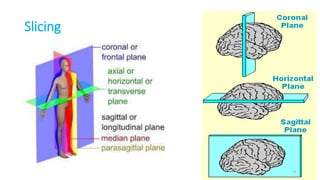
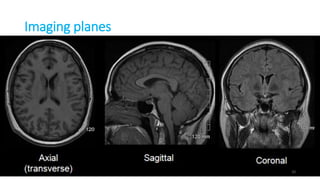
![Sagittal[s-s] Coronal[A-P] Axial[S-I]
Side view Front view Bottom up view
8](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-8-320.jpg)

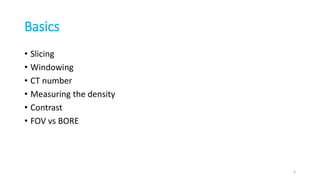
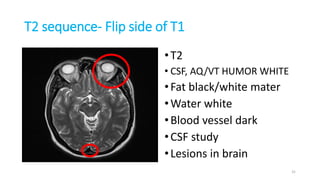
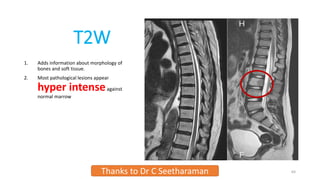
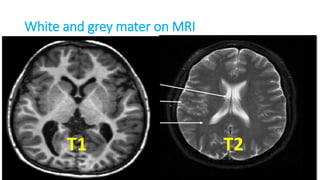
![T1 sequence
•T1
•Fat bright[white]
•Water black
•Normal anatomy
•Vascular changes
29
w w](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-29-320.jpg)

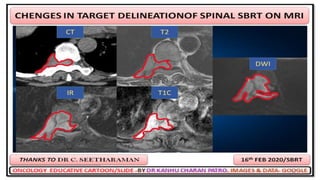
![IR sequence
1. Fat suppressed T2W sequence
2. More clear
3. Differentiate from T2 by back FAT[arrow]
1. Bright on T2
2. Darker on IR
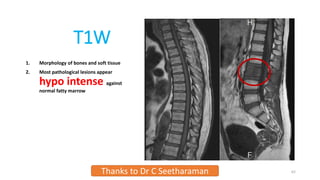
4. Most pathological lesions appear
more hyper intenseagainst normal
marrow
Thanks to Dr C Seetharaman 65
T2 SEQUENCE IR SEQUENCE](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-65-320.jpg)



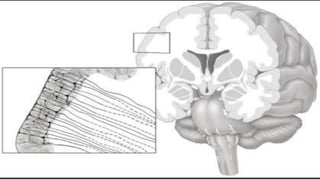
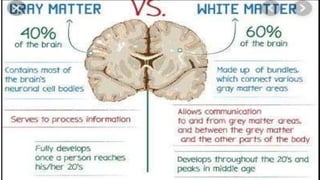
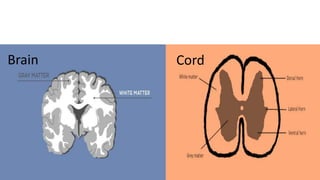
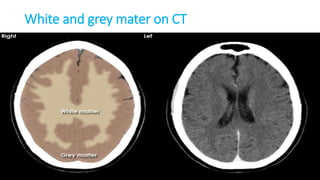
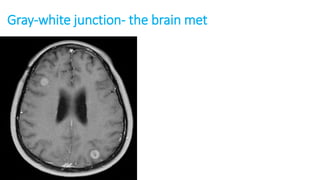
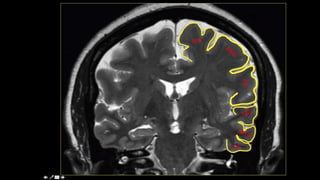
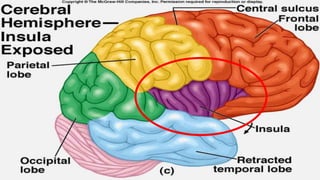
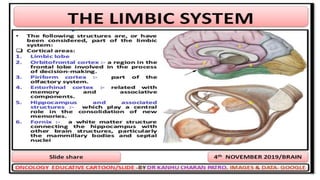
![• The CNS has two kinds of tissue: grey matter and white matter.
• Grey matter contains most of the brain's neuronal cell bodies.[outside]
• White matter is made of axons connecting different parts of grey matter to
each other[inside]](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-86-320.jpg)




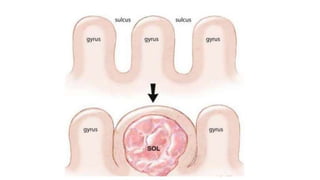
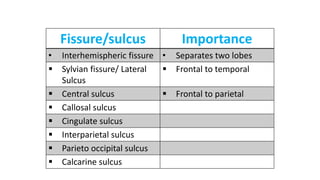
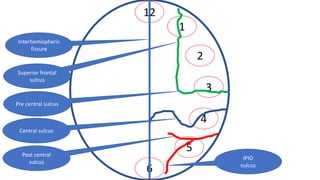
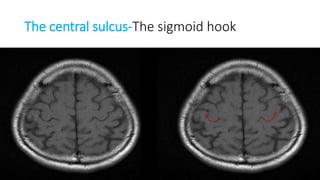
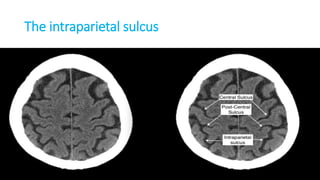
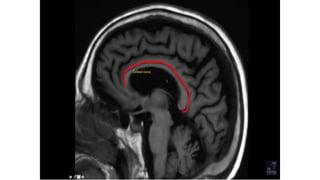
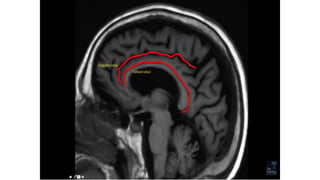
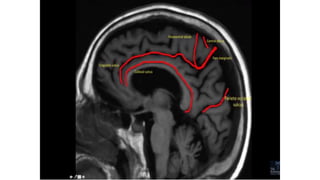
![SULCUS IS THE DEPRESSION [VALLEYS]
AND
GYRUS IS THE RIDGE [HILLS]](https://image.slidesharecdn.com/cnsradiology-200702165023/85/CNS-RADIOLOGY-FOR-RADIATION-ONCOLOGISTS-112-320.jpg)





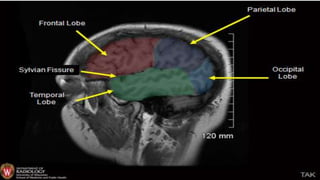
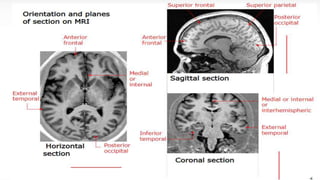
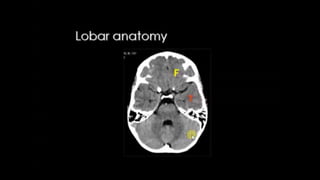
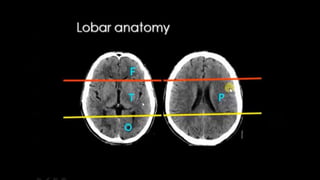
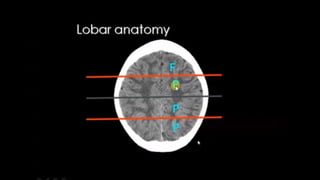
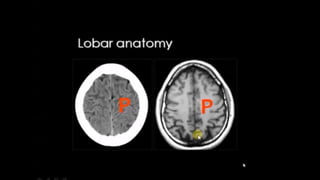
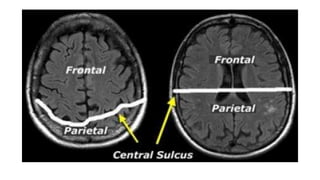
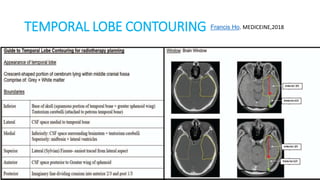
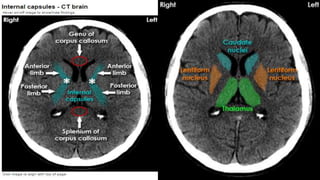
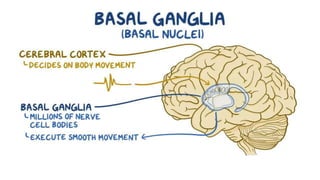



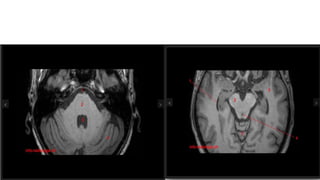
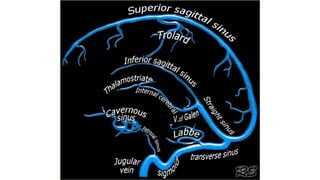
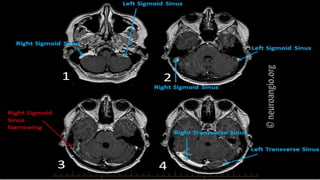
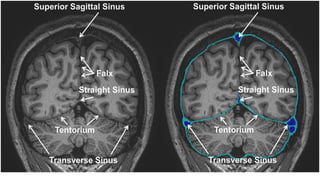
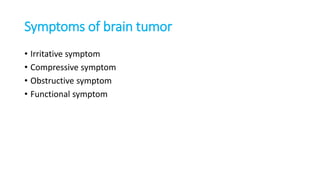


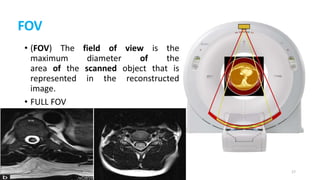
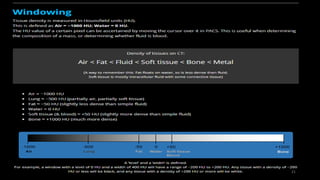
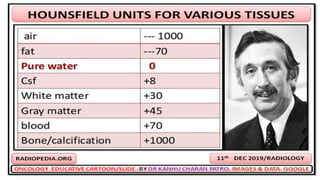
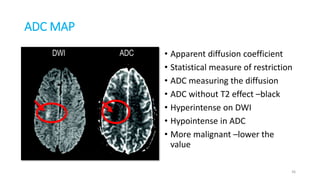
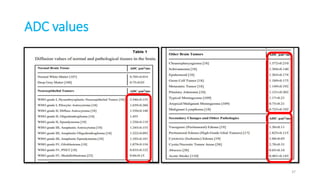
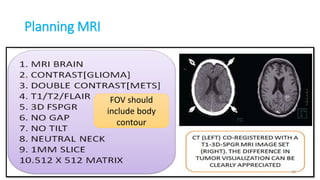
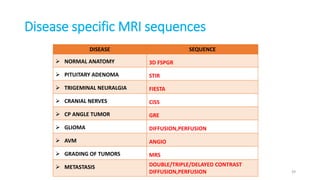
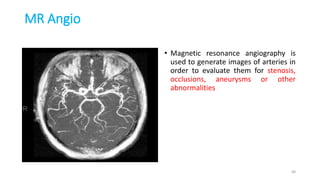
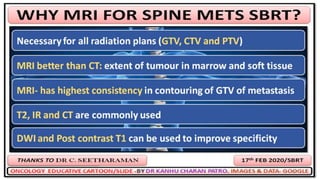
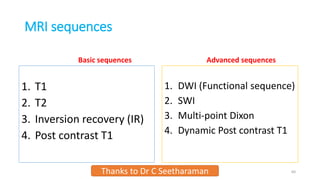
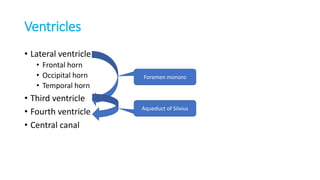
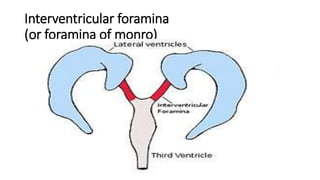
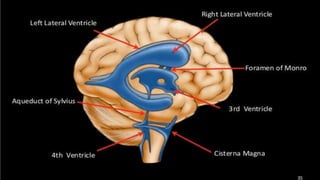
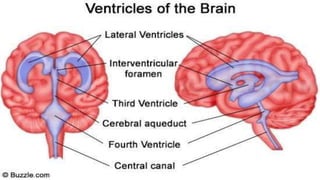
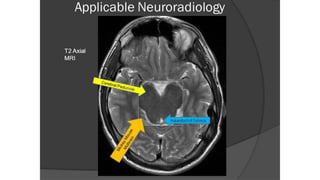
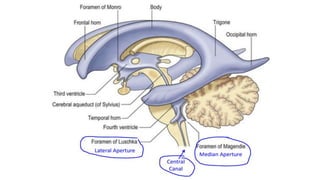
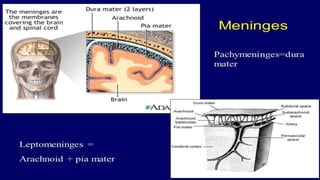
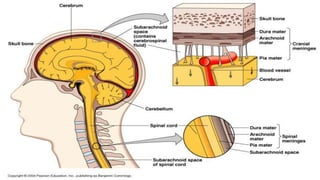
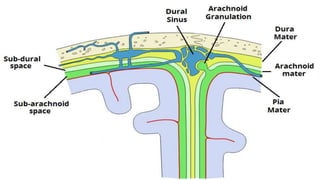
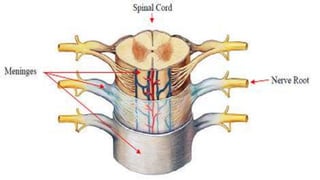
This document provides an overview of radiology for brain and spine imaging for radiation oncologists. It discusses various imaging modalities including CT, MRI, nuclear imaging and angiography. It describes key anatomical structures of the brain such as the meninges, ventricles, sulci and gyri, lobes, basal ganglia and cerebellum. Different MRI sequences are outlined including T1, T2, FLAIR, DWI and perfusion. Spine imaging including sequences for T1, T2, STIR and post-contrast are also reviewed. Important considerations for planning MRI such as field of view and disease-specific sequences are highlighted.









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













