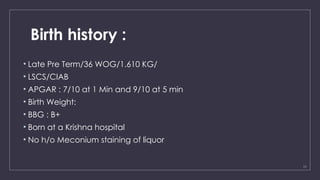
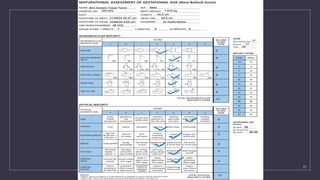
The document presents a case study of a late preterm male infant born via cesarean to a mother with no significant medical history, admitted to the NICU due to low birth weight and complications related to prematurity. The infant exhibited normal vital signs and behavior upon examination, receiving necessary immunizations and formula feeding post-birth. The overall assessment concludes the diagnosis of late preterm status with low birth weight.























![CASE PRESENTATION prev 1 lscs[1].pptxggvvvb](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationprev1lscs1-250805135156-7e04eb55-thumbnail.jpg?width=640&height=640&fit=bounds)
![CASE PRESENTATION prev 1 lscs[1].pptxgyjgg](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationprev1lscs1-250730122151-d557d04d-thumbnail.jpg?width=640&height=640&fit=bounds)









![CBME_BATCH_2023[1].pptxCBME_BATCH_2023[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cbmebatch20231-250920121332-dd14c1c1-thumbnail.jpg?width=640&height=640&fit=bounds)





















