- This is a case presentation of a 24-year-old woman, Mrs. Ranjani, who is 34 weeks and 1 day into her pregnancy. She has an Rh negative blood type while her husband's is Rh positive, making this an Rh incompatible pregnancy.
- Her past obstetric history includes one full-term vaginal delivery. During her current pregnancy she received regular antenatal checkups and her tests have been normal. She is being referred for a tertiary care opinion due to the Rh incompatibility.
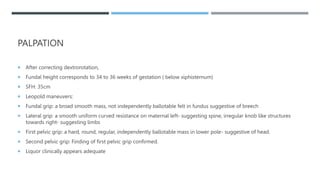
- On examination, she appears well with normal vital signs. The fetus is in a cephalic presentation with a heart rate of 146 beats per minute. Further tests and monitoring are planned to





















































![CBME_BATCH_2023[1].pptxCBME_BATCH_2023[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cbmebatch20231-250920121332-dd14c1c1-thumbnail.jpg?width=640&height=640&fit=bounds)


































