Downloaded 28 times
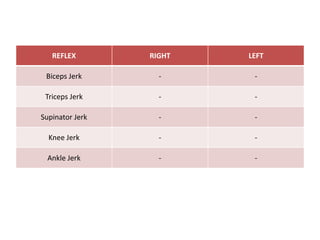
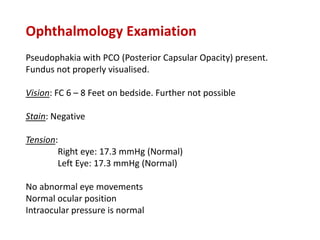
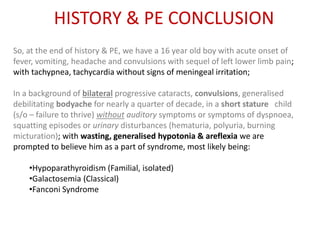
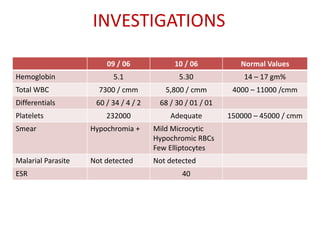
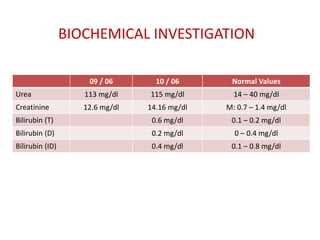
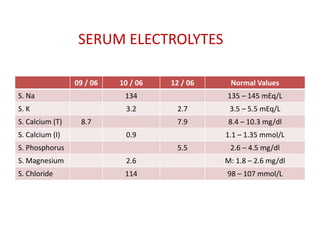
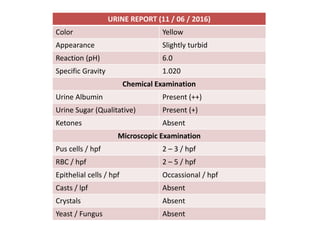
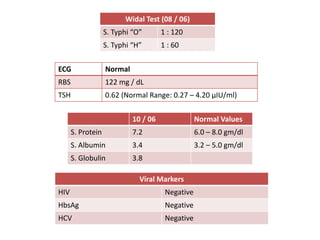
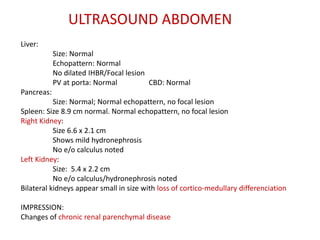
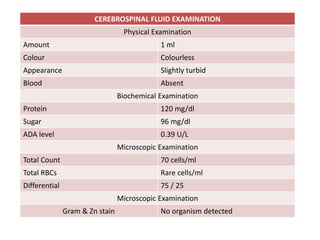
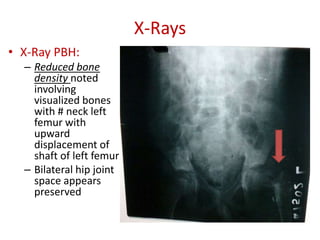
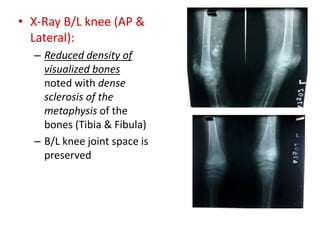

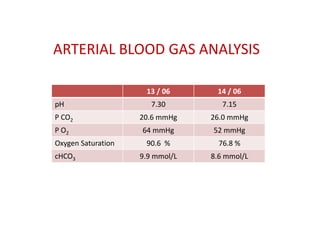
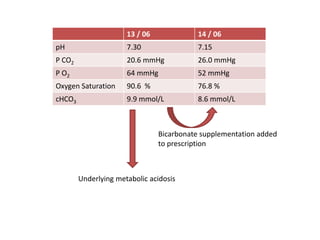
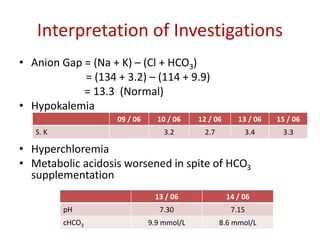
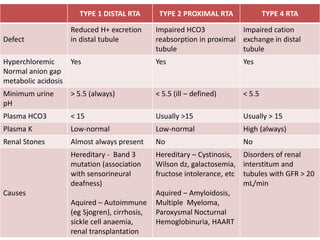
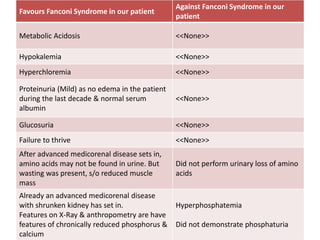


This clinical case study describes a 16-year-old boy presenting with fever, vomiting, headache, and convulsions. His past medical history is significant for bilateral cataracts, recurrent convulsions since age 10, headaches, weakness, and reduced growth. Physical exam reveals wasting, hypotonia, areflexia, and pseudophakia. Investigations show features of Fanconi syndrome including metabolic acidosis, hypokalemia, hyperchloremia, proteinuria, and glucosuria. Radiographs show reduced bone density. The constellation of findings are consistent with Lowe syndrome, a rare X-linked condition causing Fanconi syndrome, cataracts, and neurological impairment.
























































































