![Cardiac disorders manifesting as PE:
Atrial outflow obstruction:
• due to mitral stenosis or, in rare cases, atrial myxoma, thrombosis of a prosthetic
valve
• Mitral stenosis may gradually cause pulmonary edema. Other causes of CPE often
accompany mitral stenosis in acute CPE; an example is decreased LV filling because
of tachycardia in arrhythmia (eg, atrial fibrillation) or fever.
New-onset rapid atrial fibrillation and ventricular tachycardia
Acute volume overload: Ventricular septal rupture, aortic insufficiency, and
mitral regurgitation following MI
Acute exacerbation of LV systolic dysfunction:
myocardial infarction (MI)
Patient noncompliance with dietary restrictions (eg, dietary salt restrictions)
Patient noncompliance with medications (eg, diuretics)
Severe anemia
Sepsis
Thyrotoxicosis
Myocarditis
Myocardial toxins (eg, alcohol, cocaine, chemotherapeutic agents such as Adriamycin]](https://image.slidesharecdn.com/clinicalassessment2-151030122926-lva1-app6891/85/Clinical-assessment-part-2-17-320.jpg?cb=1709450623)
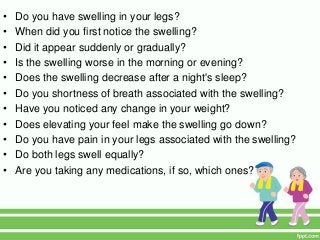
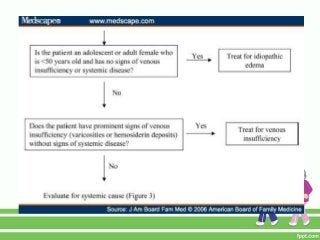
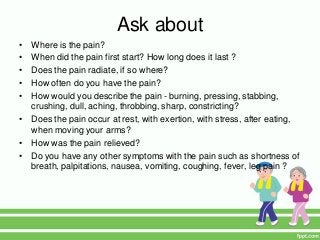
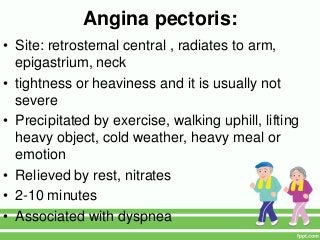
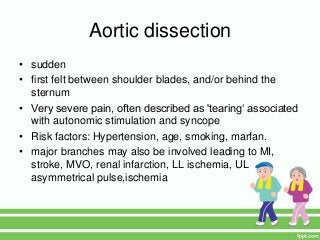

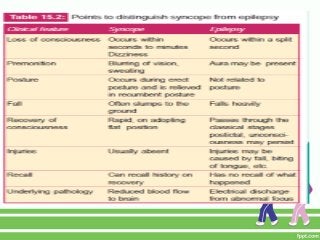
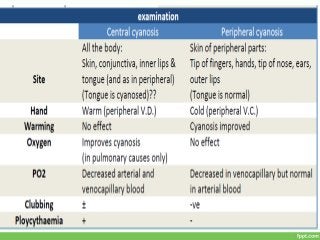


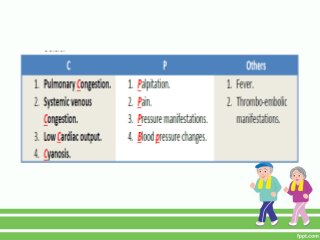
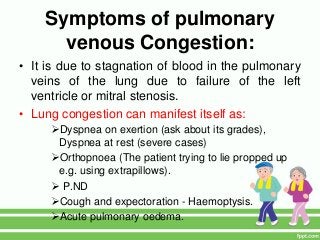
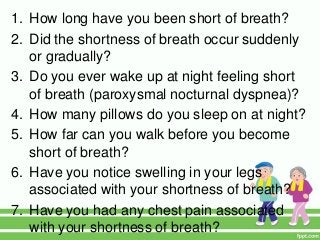
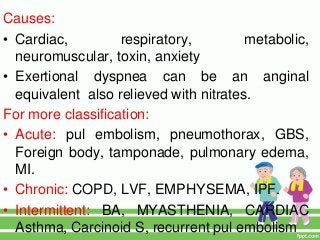
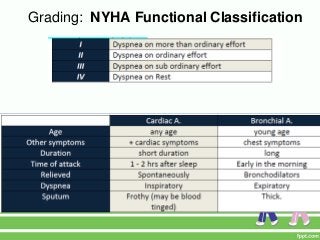
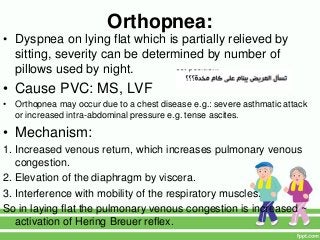
This document provides guidance on assessing symptoms related to cardiac issues in geriatric patients. It discusses how to evaluate dyspnea, cough, palpitations, chest pain, leg swelling, and other symptoms by asking about duration, onset, precipitating/relieving factors, and associated symptoms. Specific questions are provided to assess orthopnea, paroxysmal nocturnal dyspnea, hemoptysis, edema, and different types of chest pain. Causes and characteristics of different conditions like pulmonary venous congestion, acute pulmonary edema, and low cardiac output are also summarized.



























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








