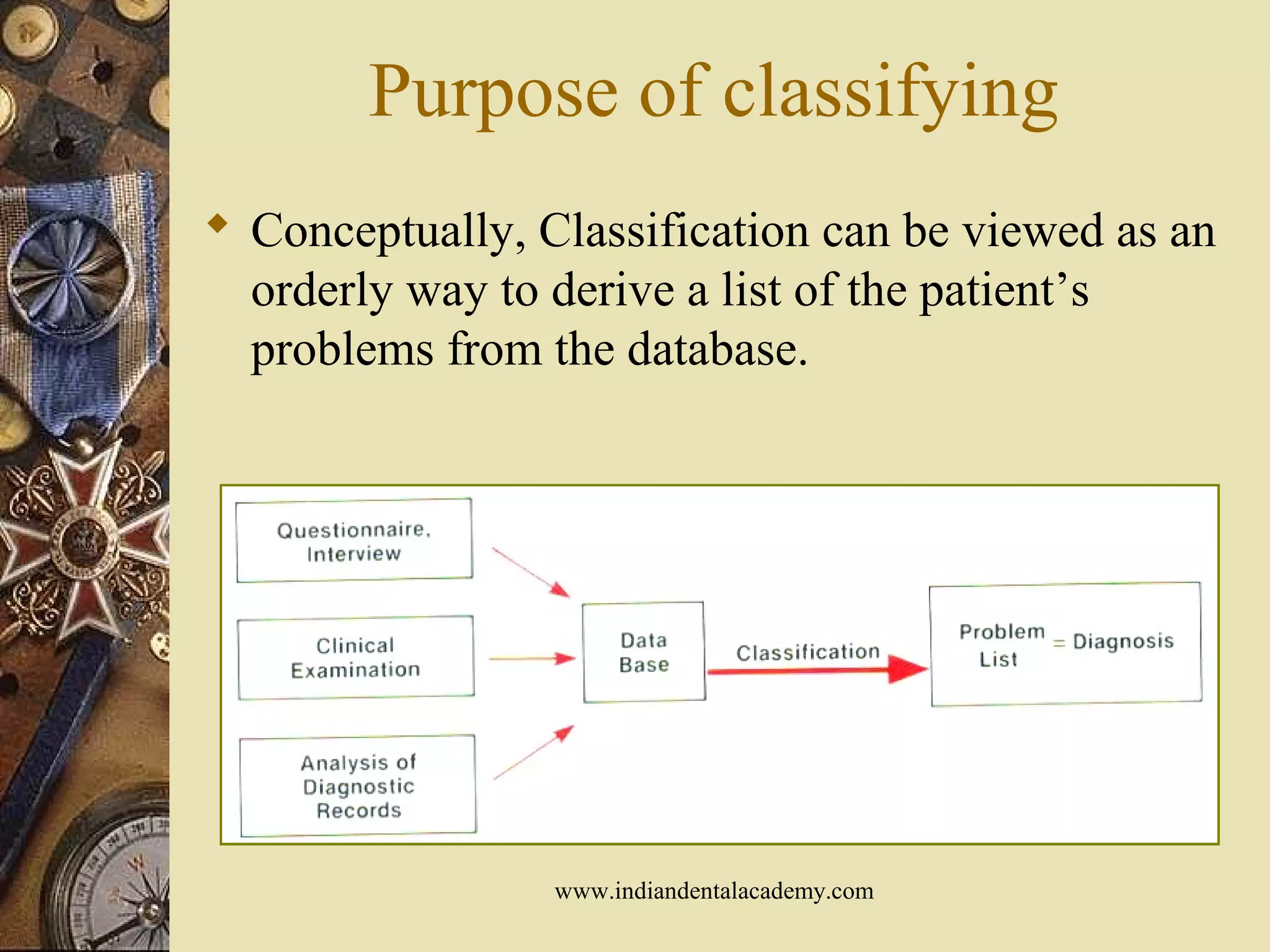

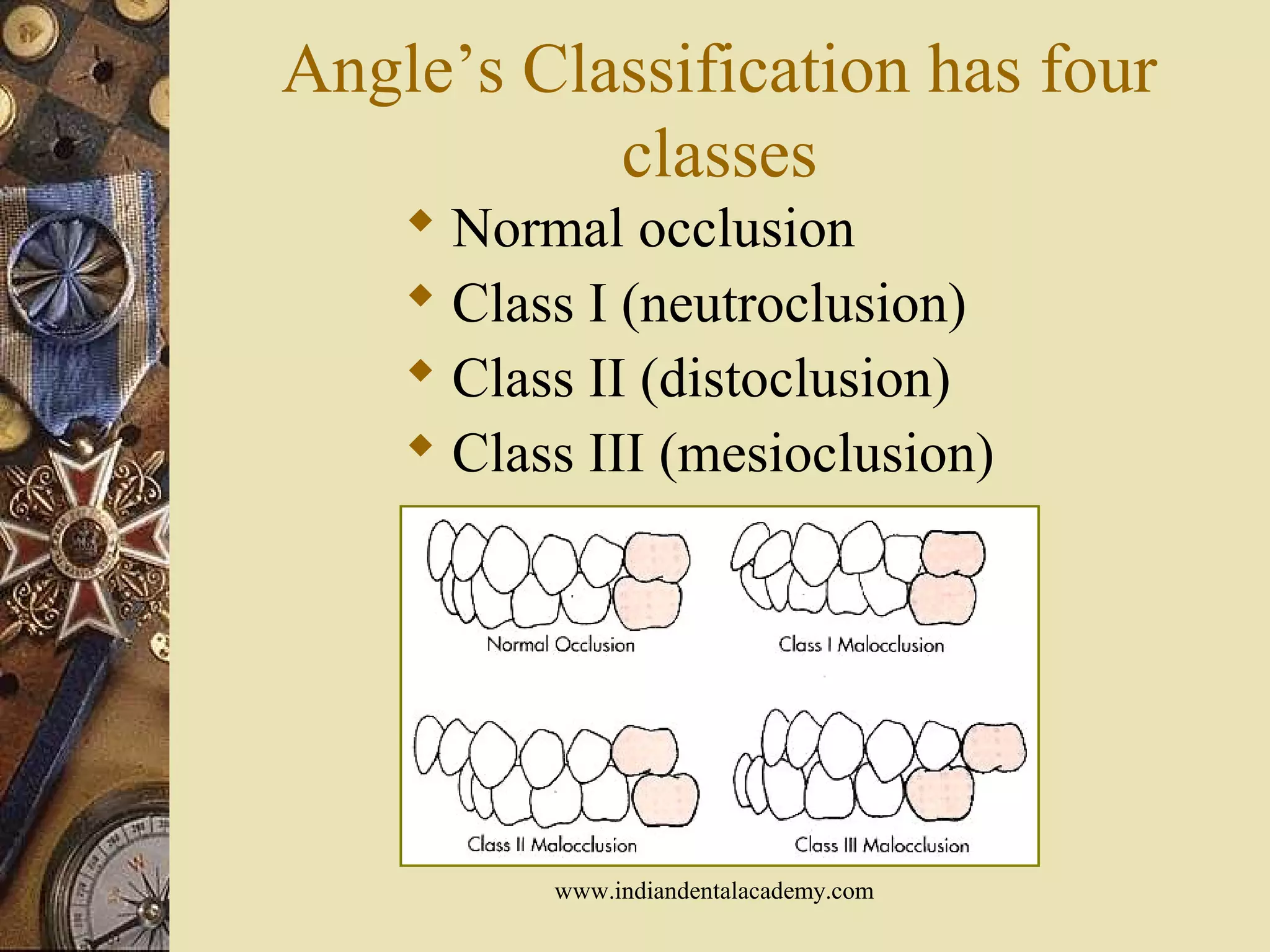
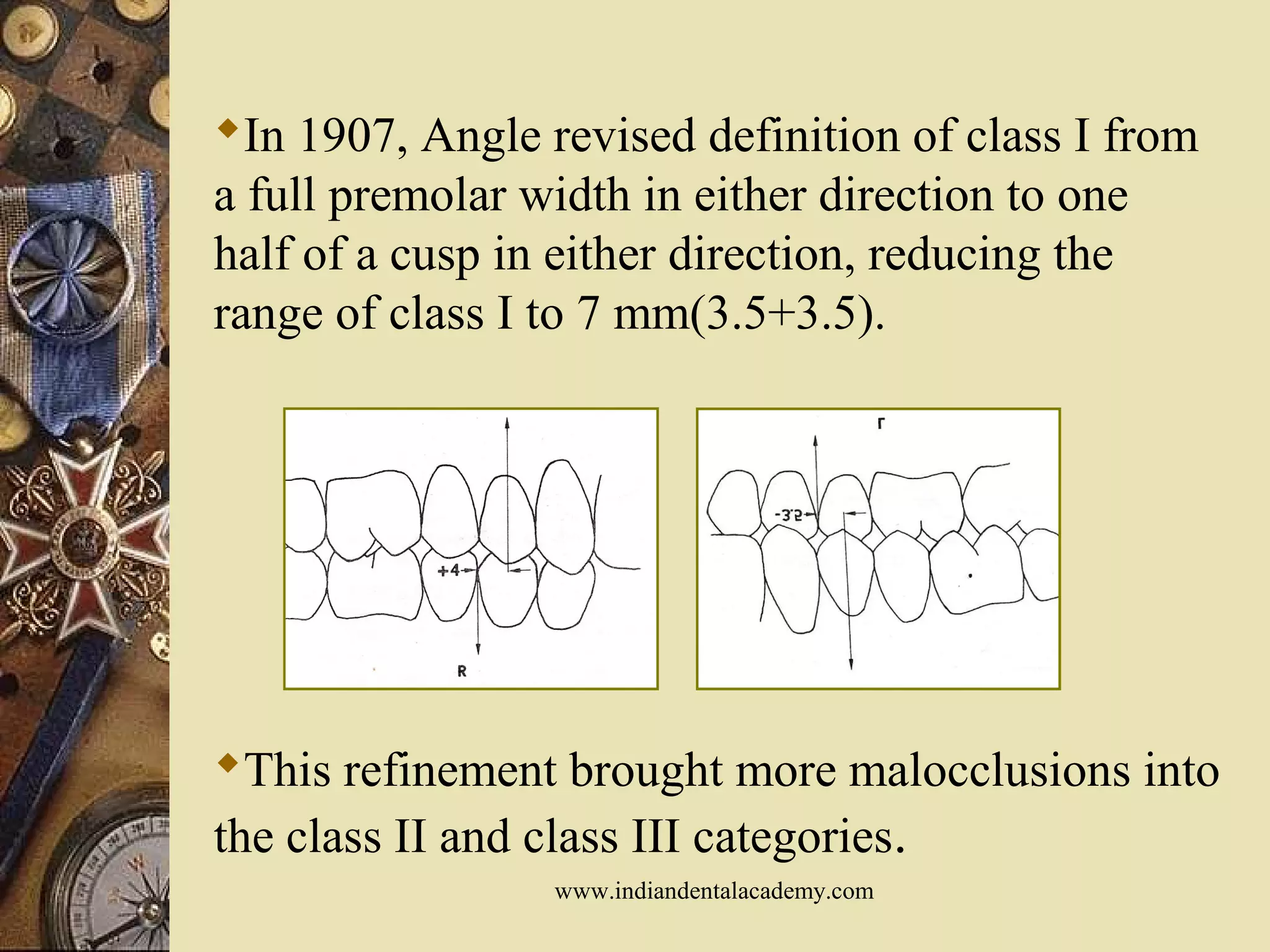
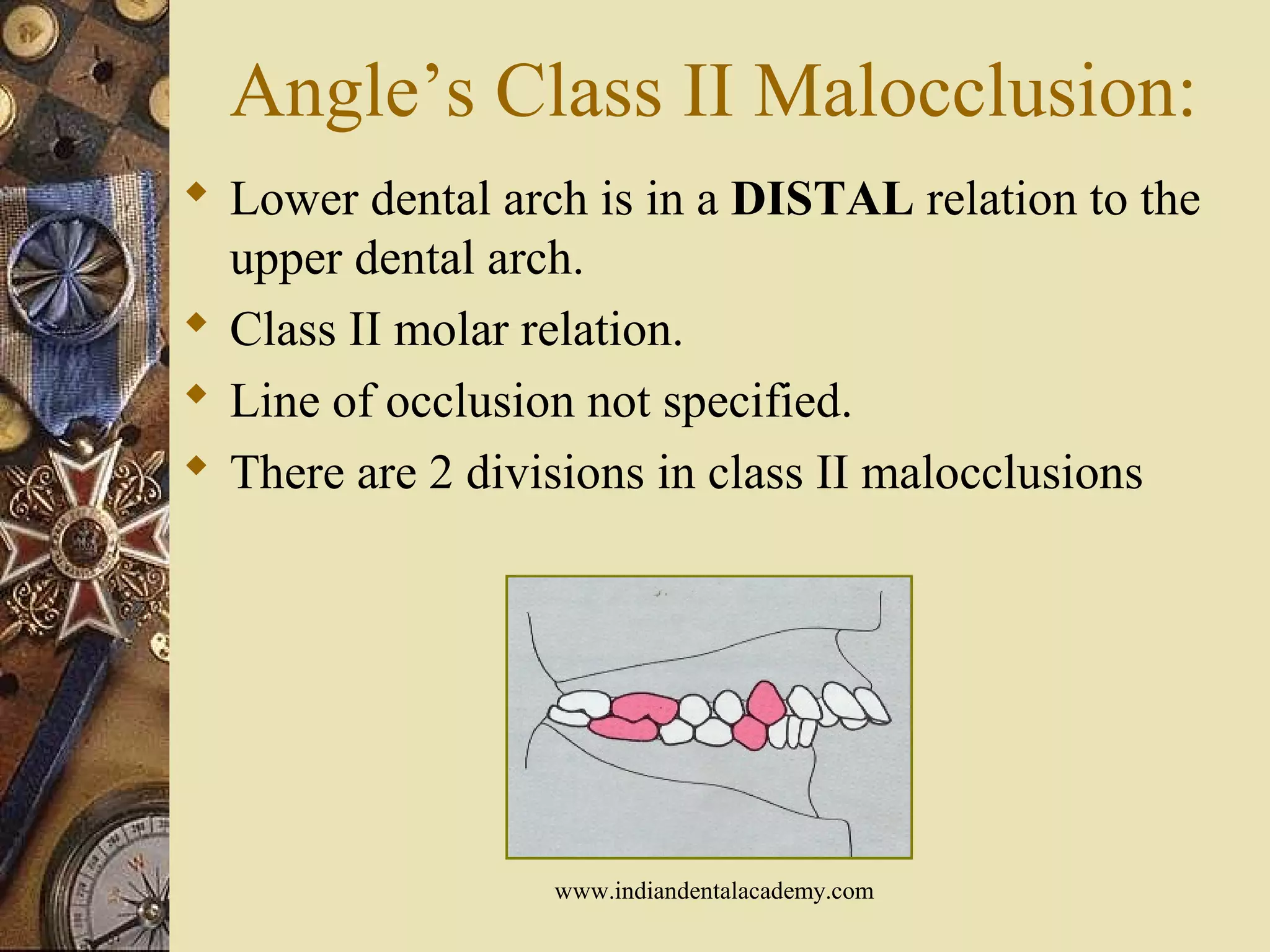
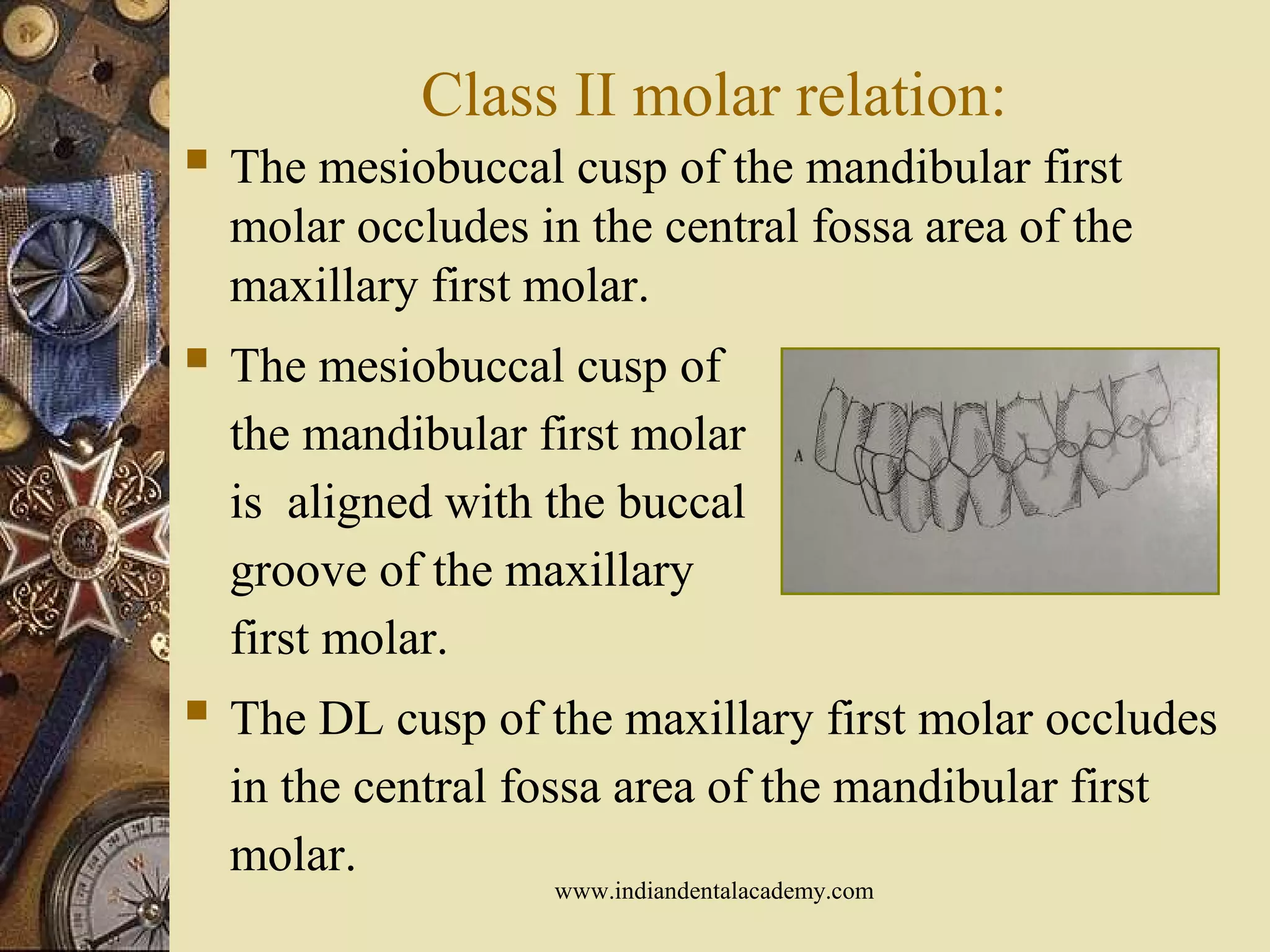
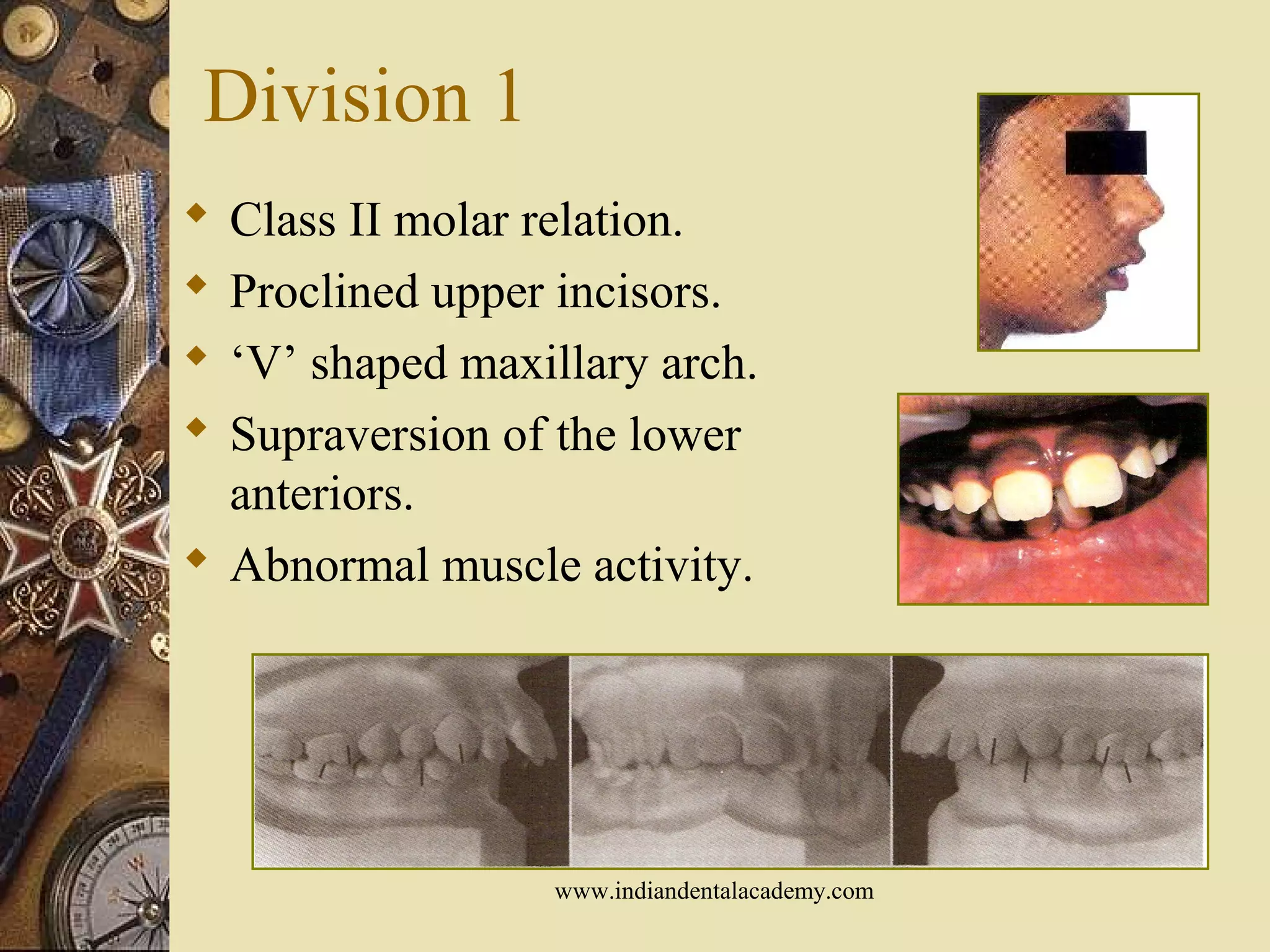
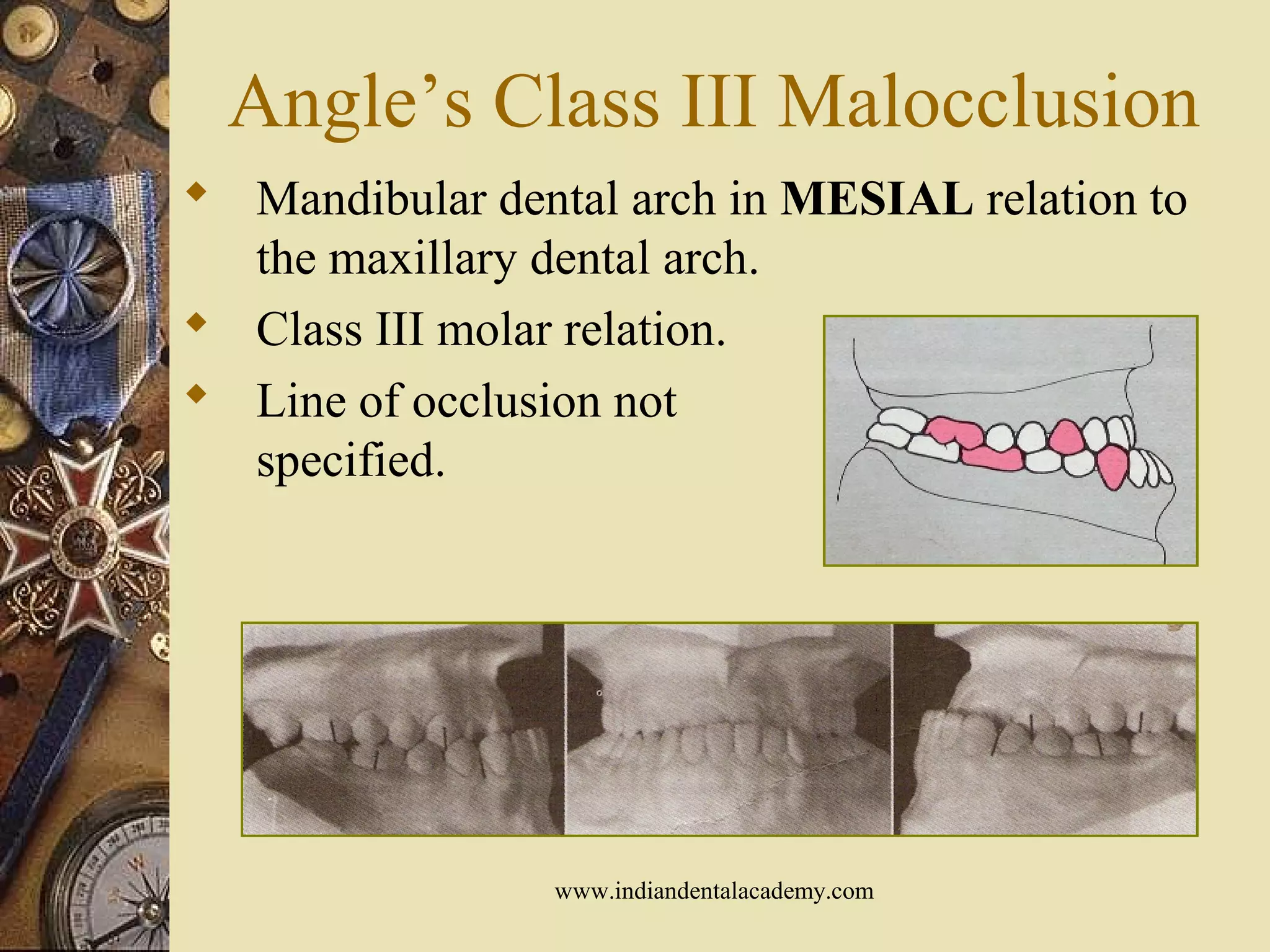
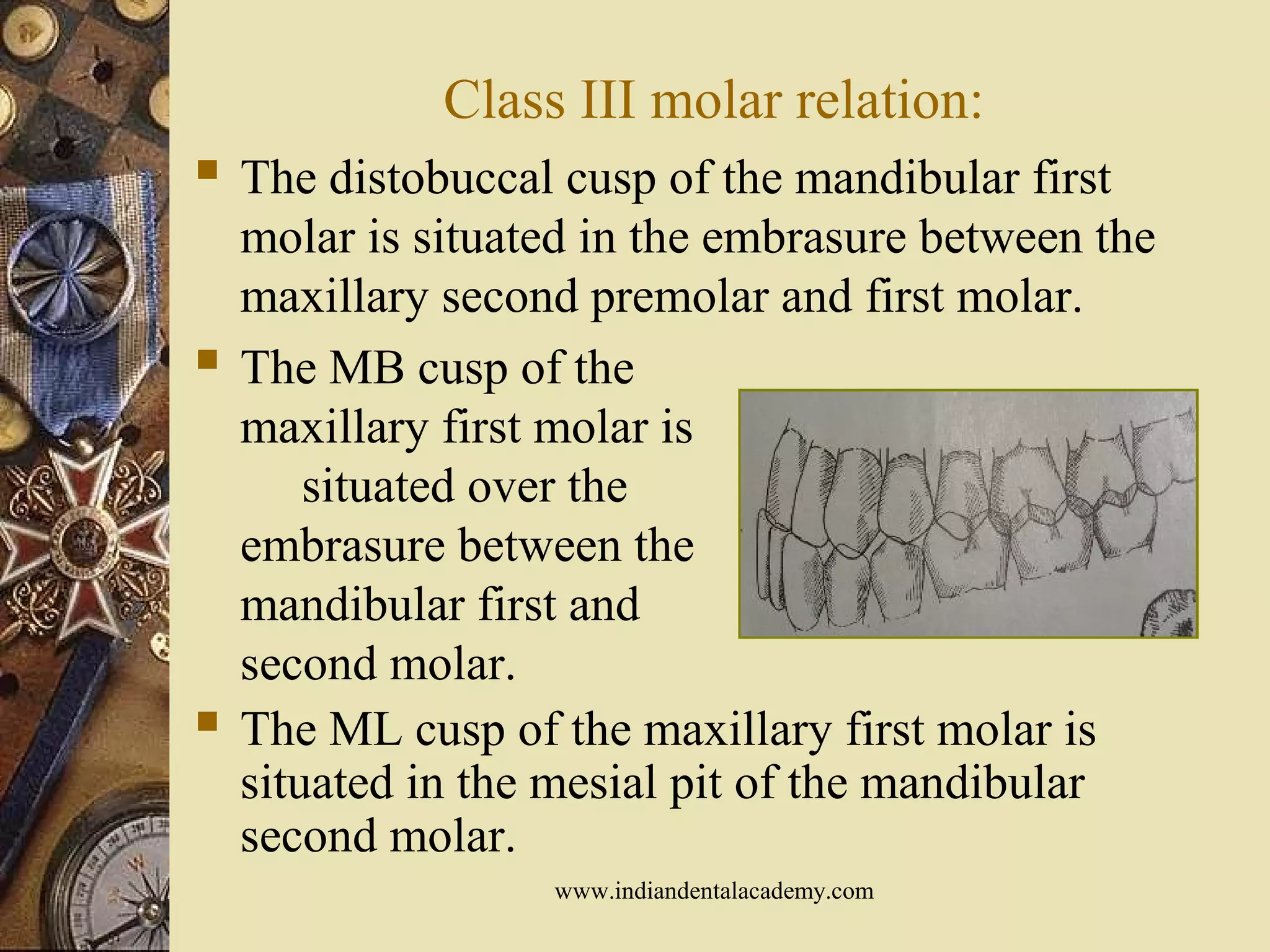

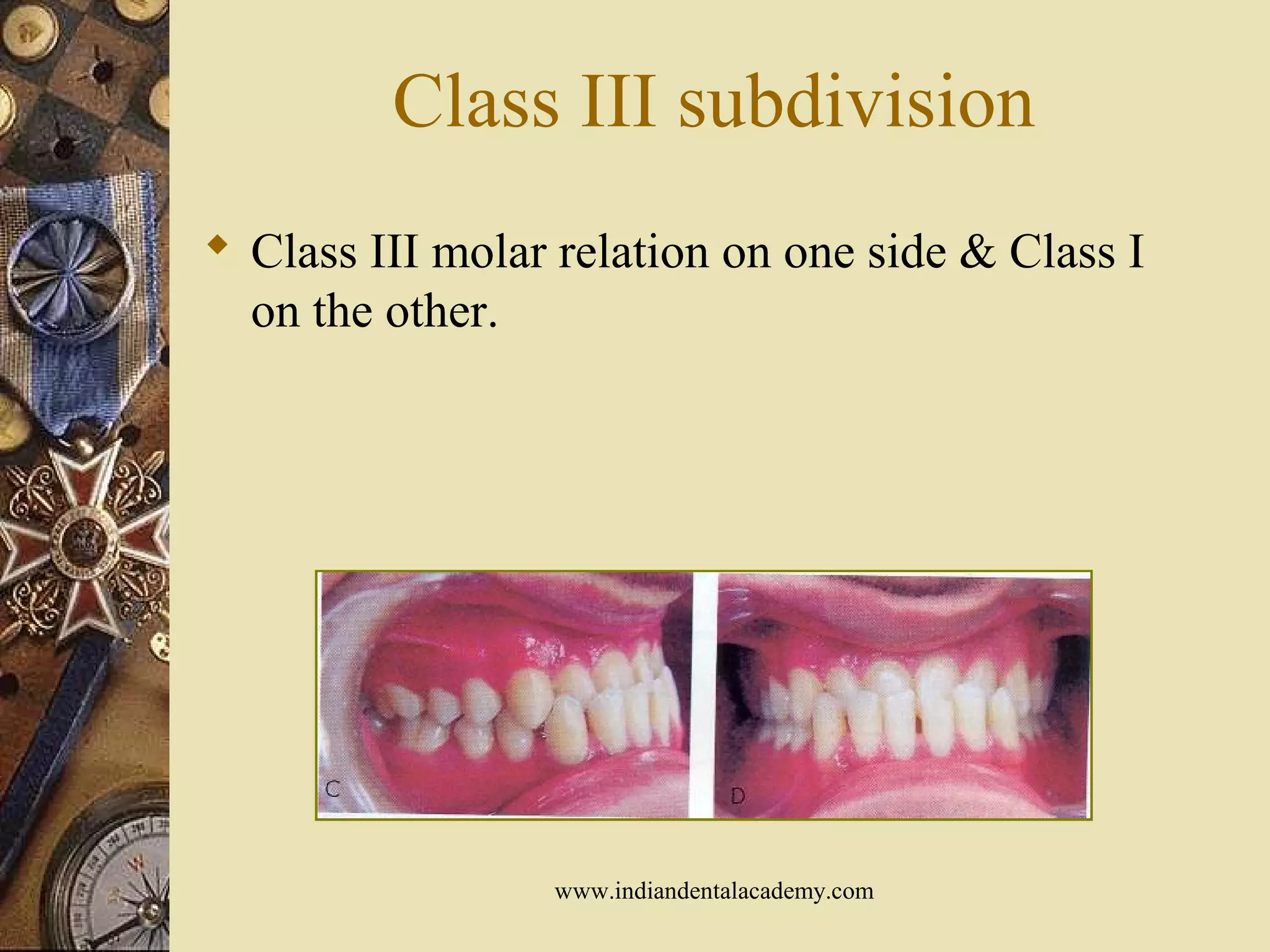
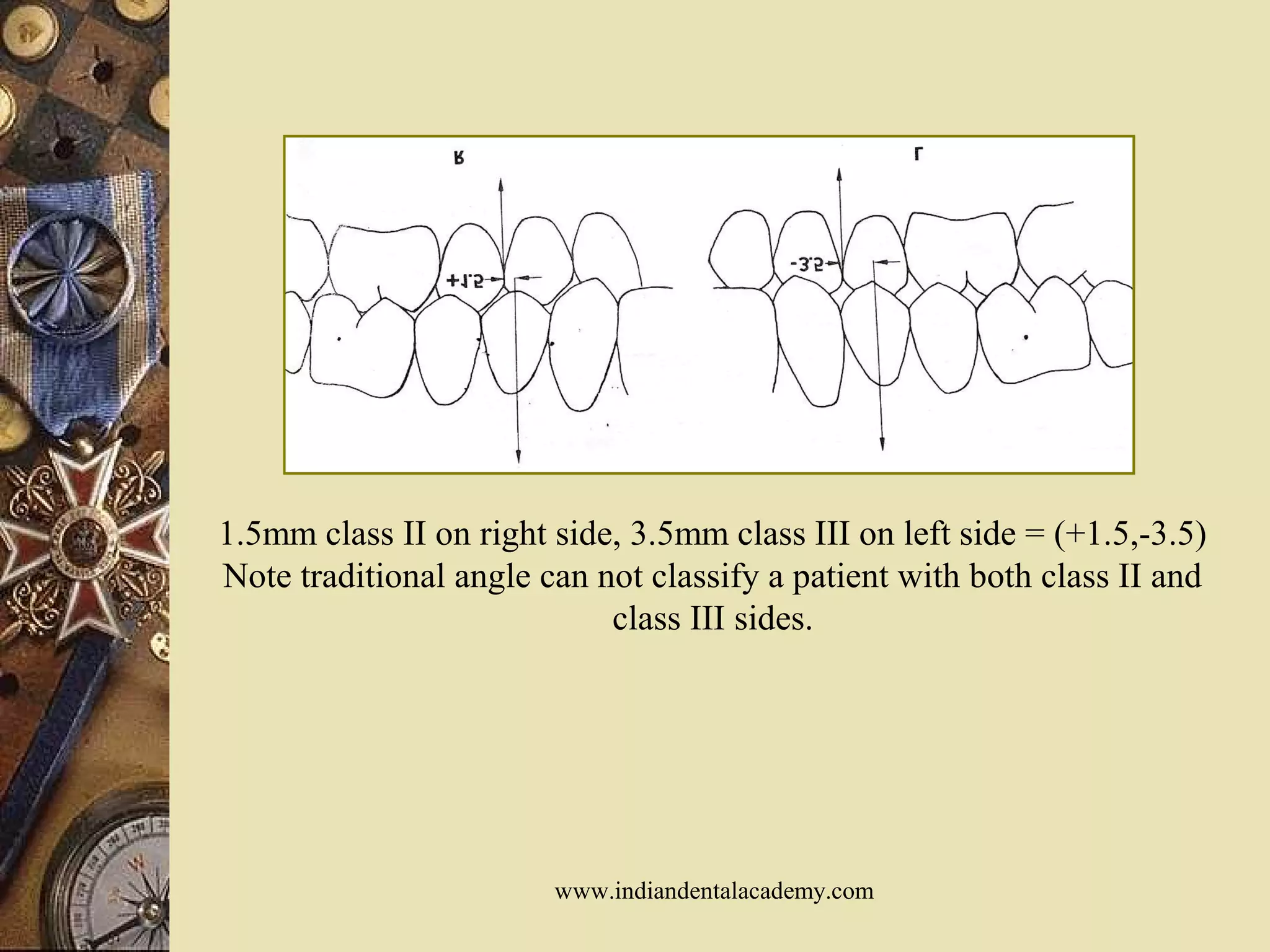


The document discusses various classification systems for malocclusion, primarily focusing on Angle's classification, which categorizes malocclusions into Class I, Class II, and Class III based on the relationship of the first molars. It outlines the purpose and need for classification, advantages and disadvantages of the systems, along with several modifications and alternative classifications, emphasizing their significance in orthodontics. The document concludes by addressing the need for precise goals in orthodontic treatment and discusses Moyer's etiologic classification based on tissue origin.

































































































