










![3. Facial Axis of the Clinical Crown
[FACC]
For all the teeth except molars, the most
prominent portion of the central lobe on each
crown’s facial surface. For molars, buccal
groove that separates the 2 large facial
cusps.
4. FA Point
The point on the facial surface that
separates the gingival half of the
clinical crown from the occlusal
half www.indiandentalacademy.com](https://image.slidesharecdn.com/andrewssixkeysofocclusion-160507065646/75/Andrews-six-keys-of-occlusion-certified-fixed-orthodontics-courses-in-india-22-2048.jpg)




















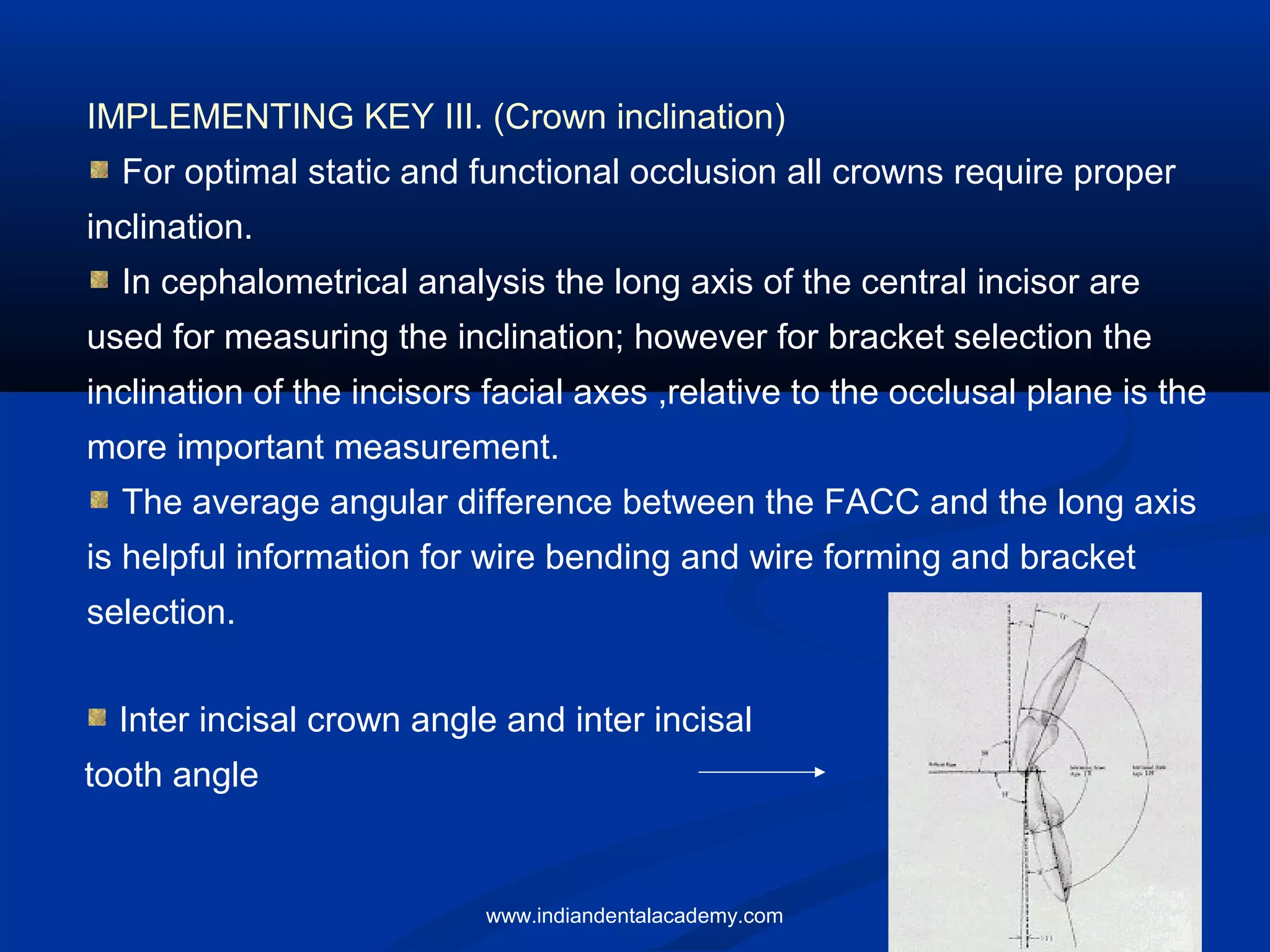

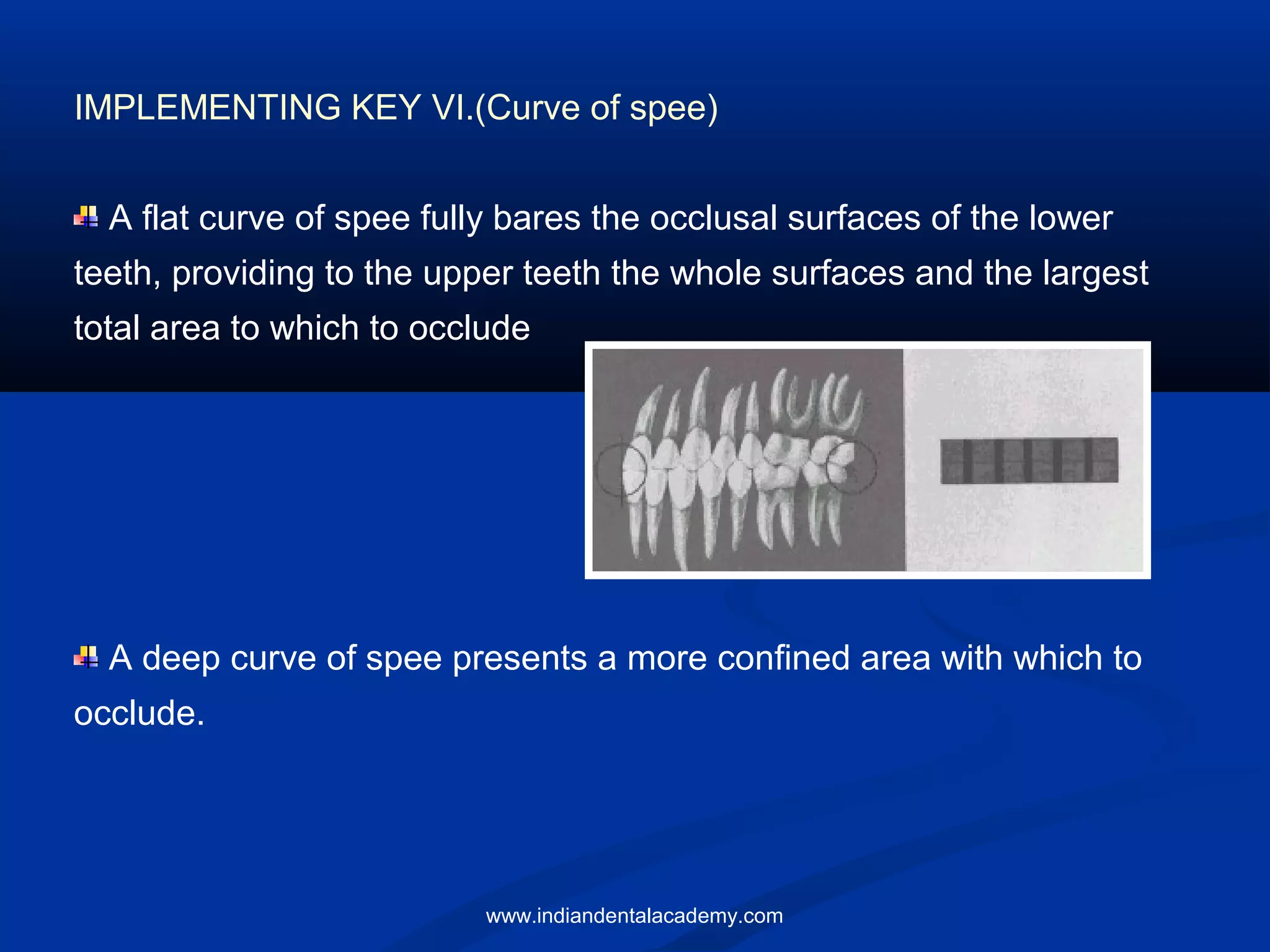



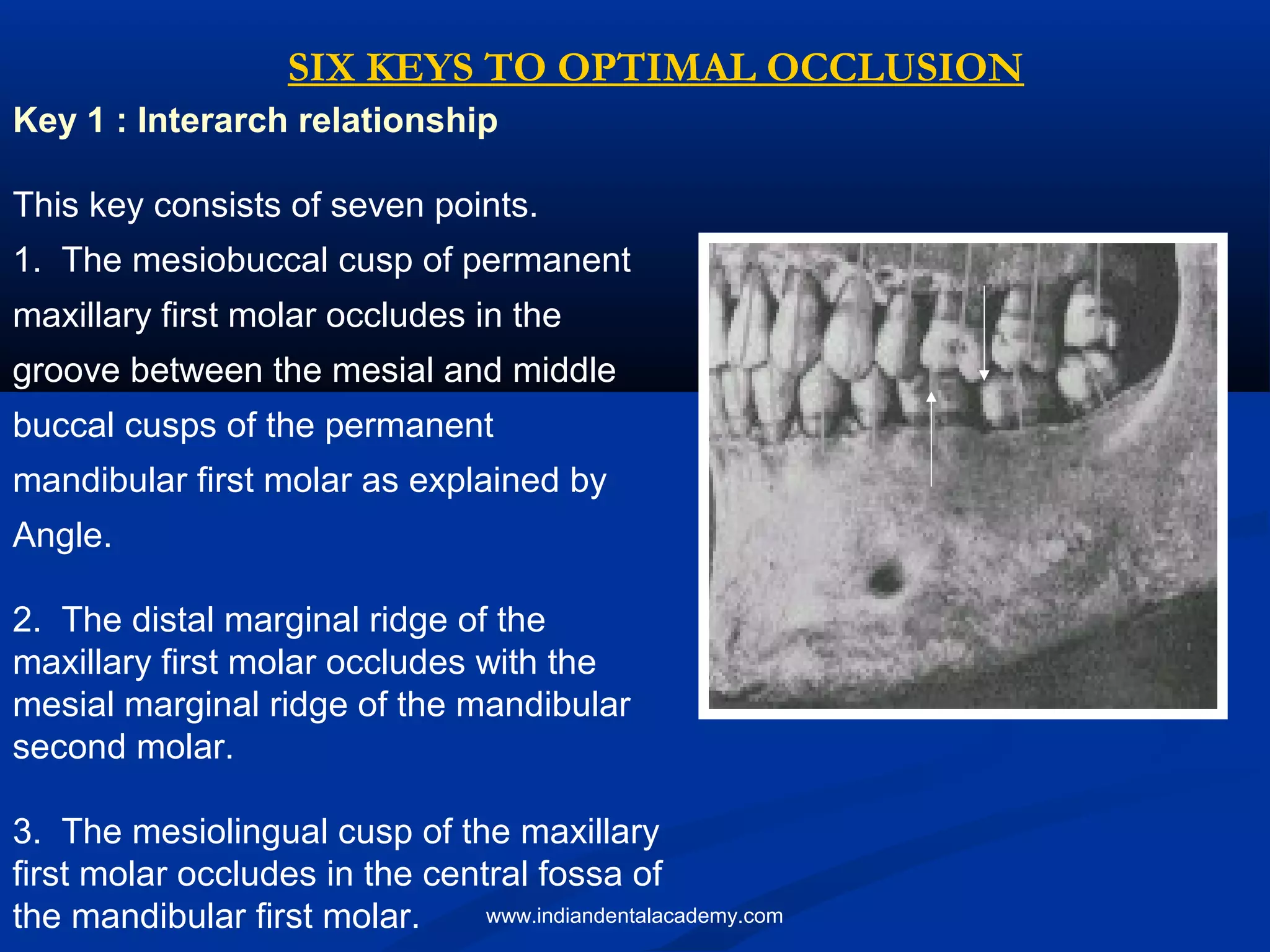
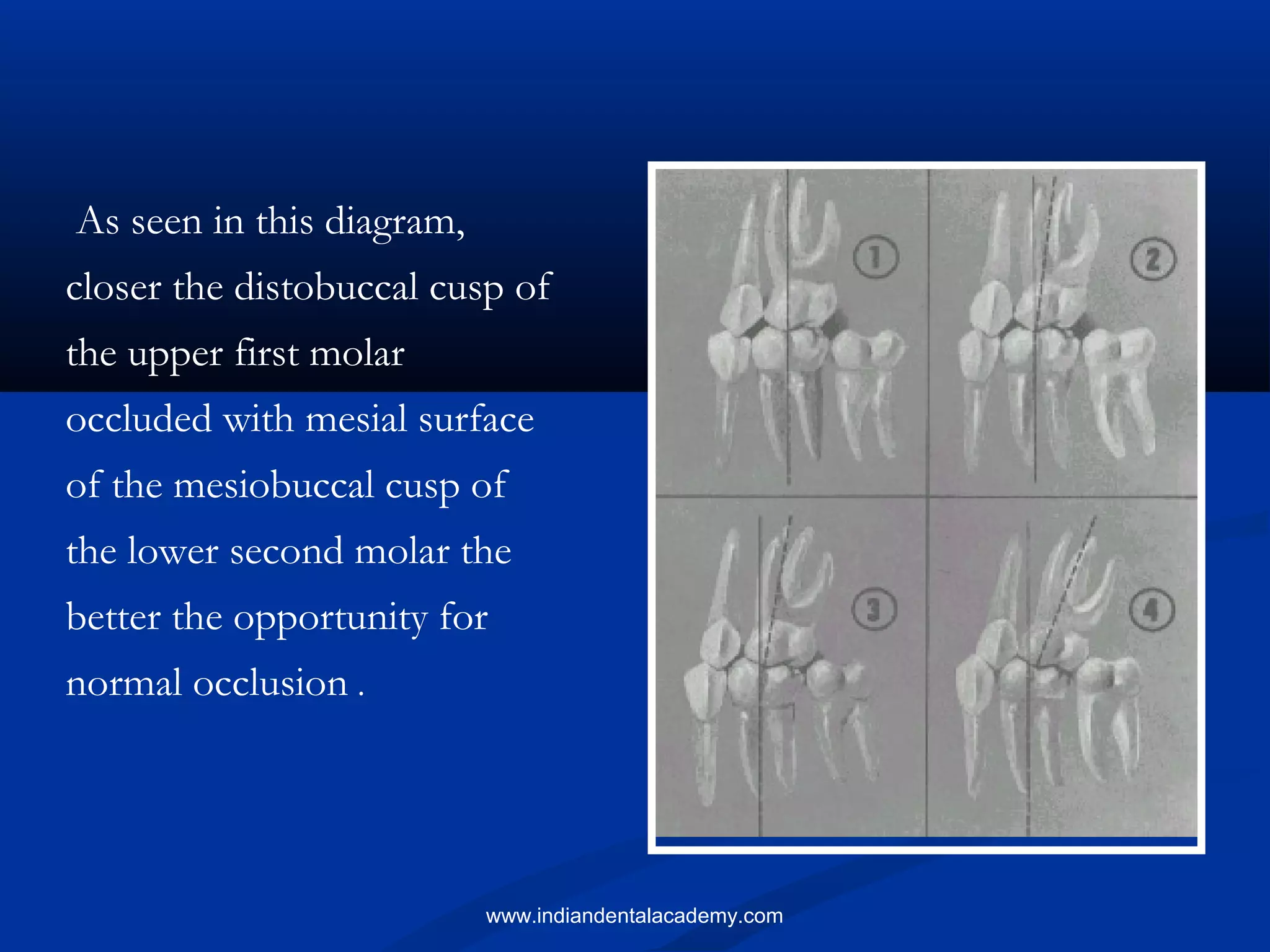
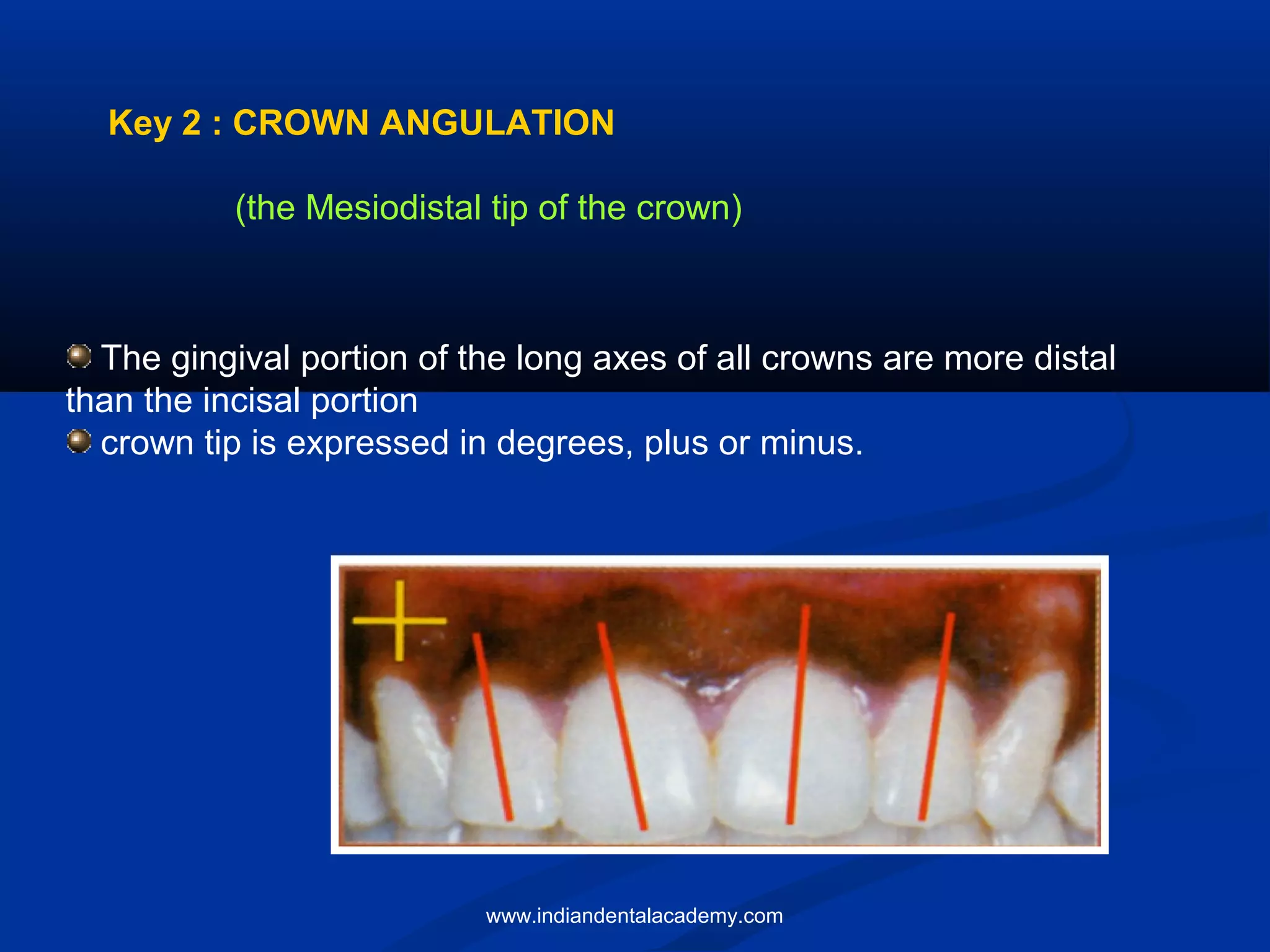
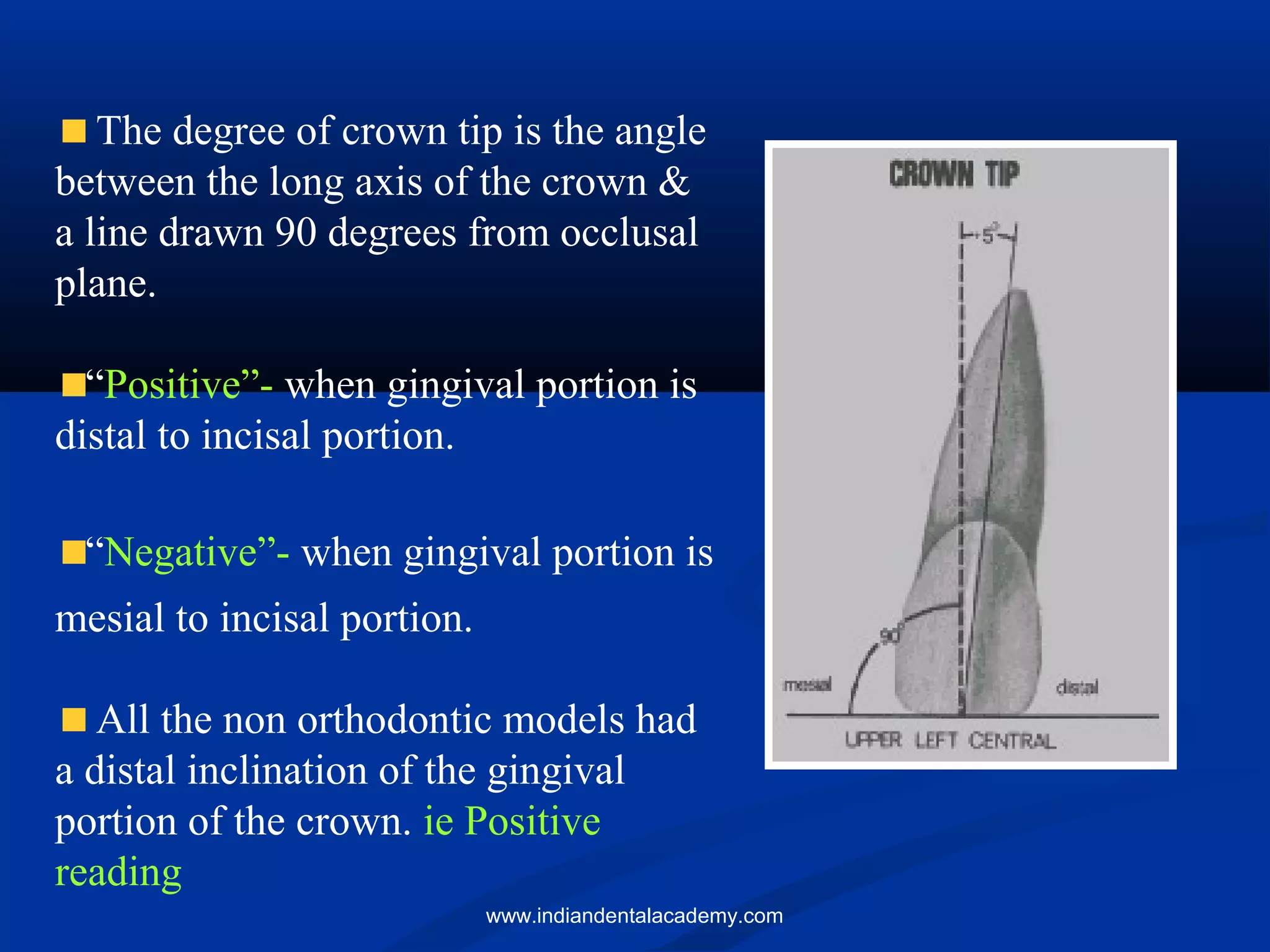
The document discusses orthodontic occlusion and presents six keys to optimal occlusion identified by Lawrence F. Andrews based on his research of 120 non-orthodontic dental models. These keys serve as important indicators for proper diagnosis and treatment planning in orthodontics, emphasizing the significance of inter-arch relationships, crown angulation, inclination, rotations, tight contacts, and occlusal planes. Andrews' study contrasts naturally optimal occlusions with treated cases to highlight shortcomings in traditional orthodontic methods.























































































