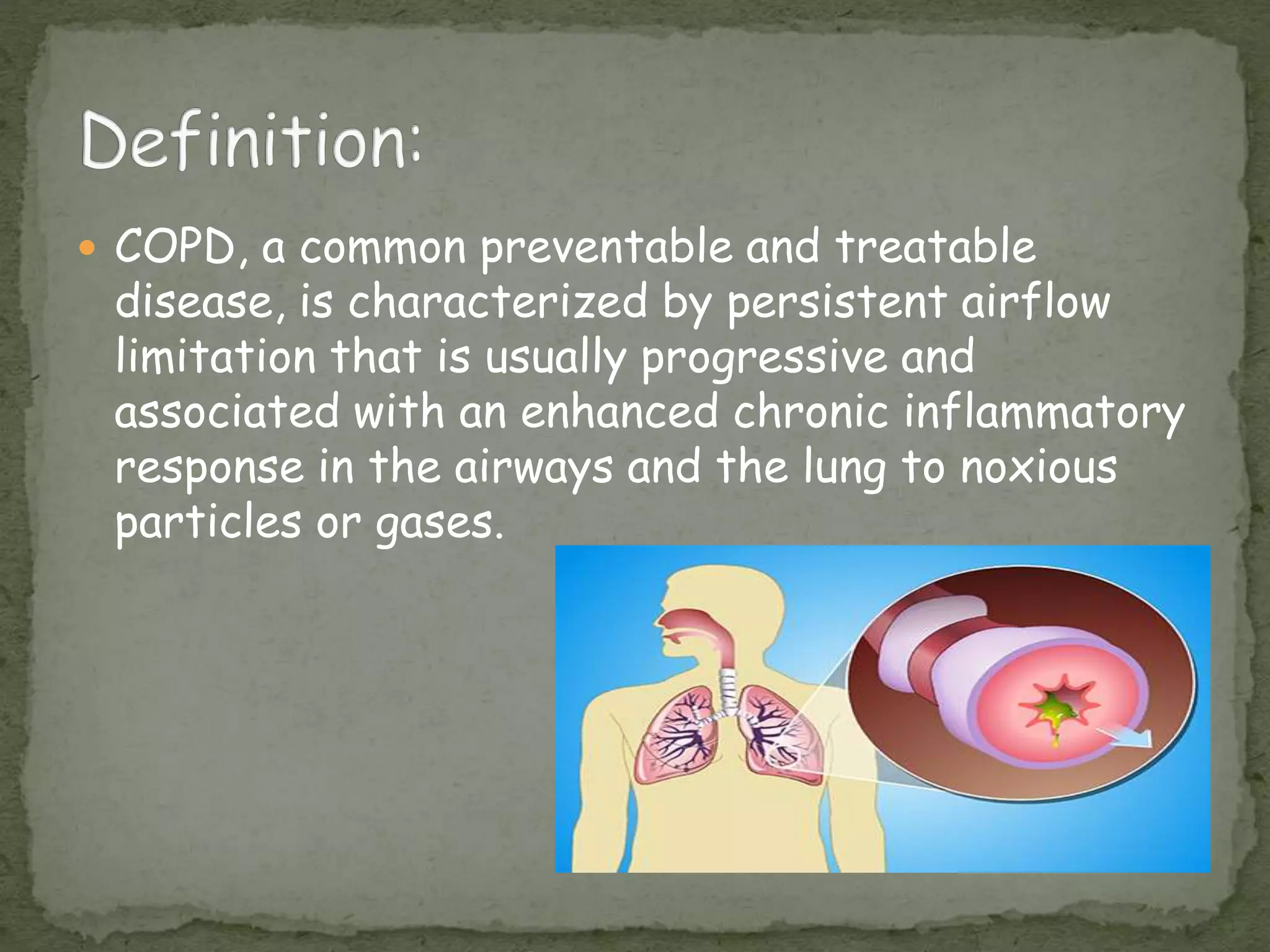
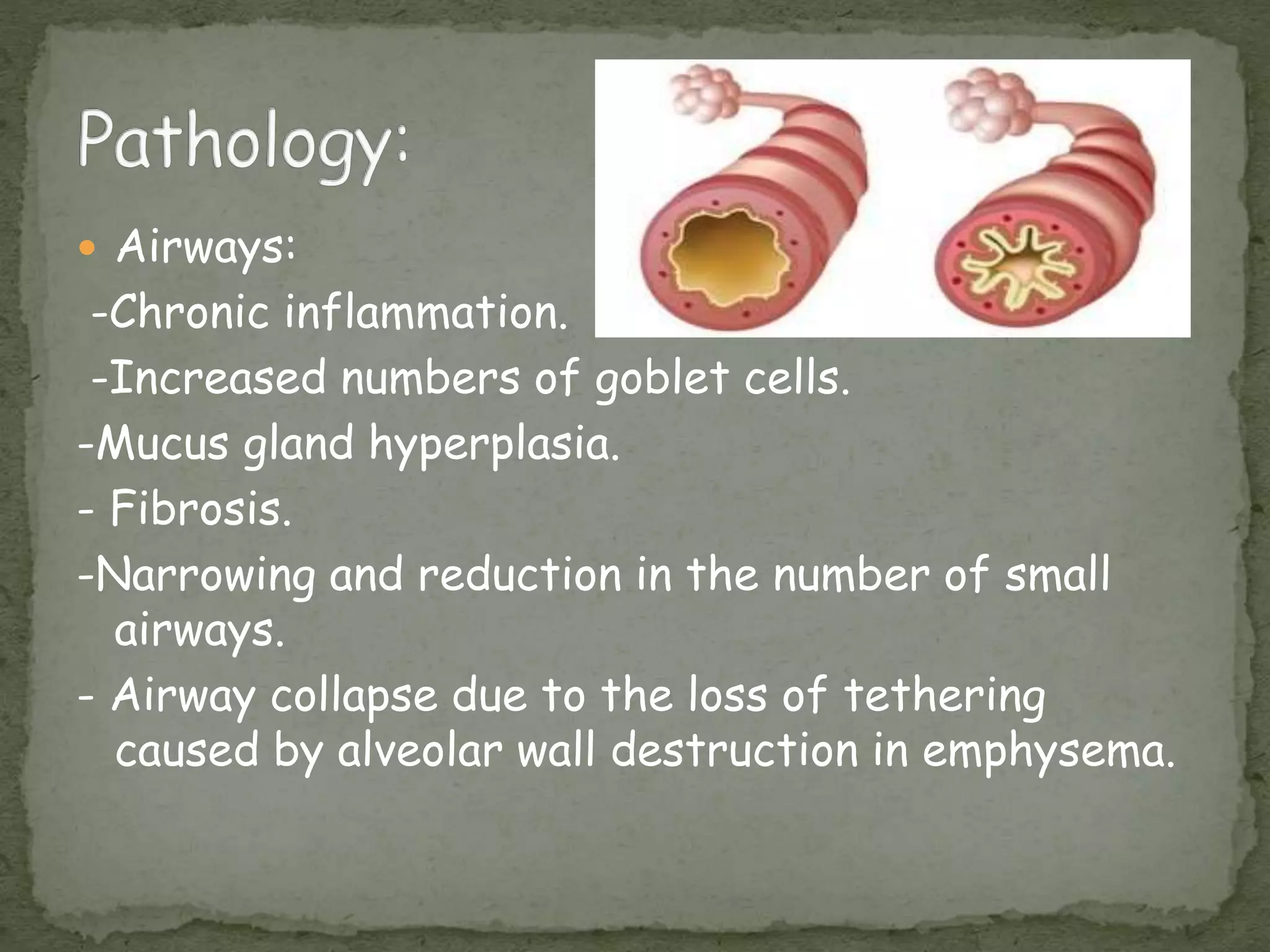
COPD is a common lung disease characterized by persistent airflow limitation caused by damage to the lungs, usually from smoking. It is the fourth leading cause of death. Symptoms include shortness of breath, chronic cough, and sputum production. Diagnosis is confirmed by pulmonary function tests showing airflow limitation that is not fully reversible. Treatment focuses on reducing symptoms and exacerbations through bronchodilators, inhaled corticosteroids, pulmonary rehabilitation, oxygen therapy, and managing comorbidities.