Downloaded 1,040 times

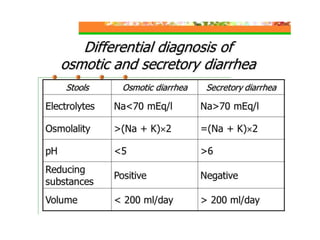








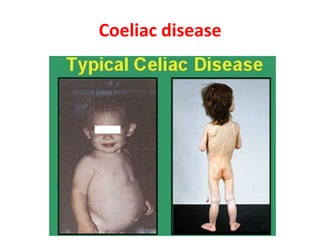








This document discusses chronic diarrhea in children, including definitions, causes, diagnosis, and treatment. It defines chronic diarrhea as diarrhea lasting 2-3 weeks or more. Common causes in infants include post-infectious lactase deficiency, celiac disease, cow's milk allergy, toddler's diarrhea, and infections like giardiasis. Diagnosis involves taking a thorough history and physical exam, with investigations tailored to the child's age and suspected causes, such as stool exams and tests for carbohydrate malabsorption.





















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









