Downloaded 258 times

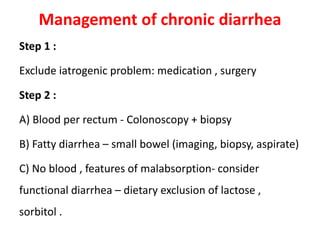
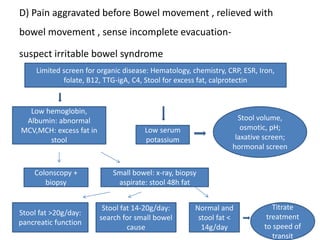
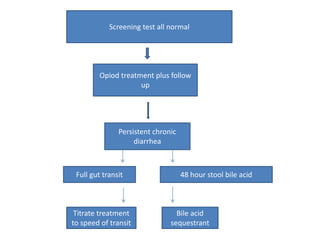


1. Chronic diarrhea is defined as persistent changes in stool consistency and increased stool frequency lasting over 4 weeks. 2. The causes of chronic diarrhea include secretory, osmotic, steatorrheal, inflammatory, dysmotility, and iatrogenic factors. 3. The approach to a patient with chronic diarrhea involves obtaining a detailed history and physical exam, followed by screening tests and further testing depending on the results to identify the underlying cause and guide management.









































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






