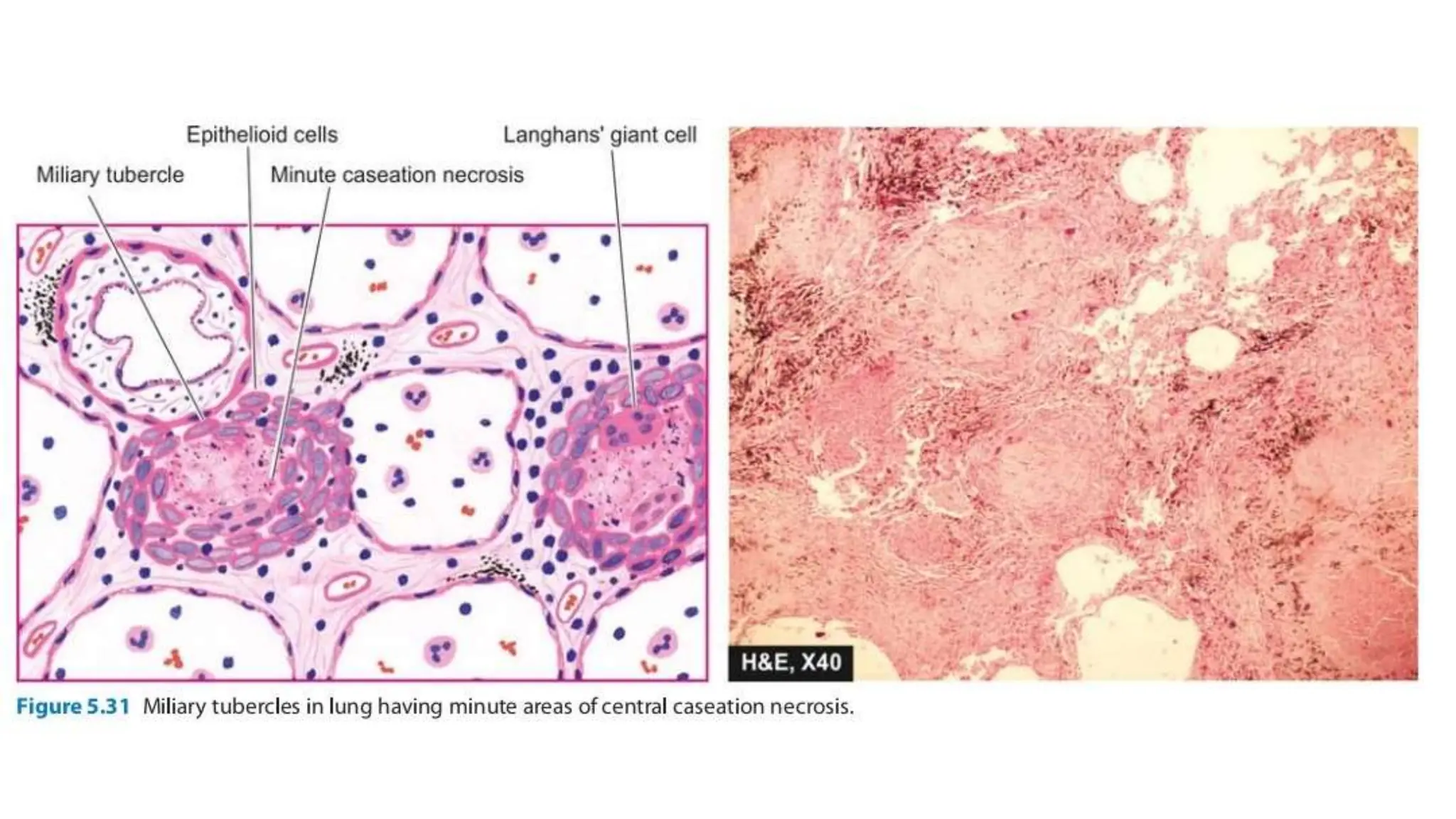
The document provides an overview of respiratory system anatomy and tuberculosis, detailing the structure and function of the lungs and the characteristics of Mycobacterium tuberculosis. It explains the modes of transmission, types of tuberculosis (primary and secondary), and the associated lymphatic spread and complications. Key clinical features and pathology of tuberculosis lesions, including Ghon complex and granuloma formation, are also discussed.