Download as PDF, PPTX

![Is Bangalore in the grip of chikungunya?
[ Saturday, A il 08 2006 12 33 46 am TIMES NEWS
S t d April 08, 12:33:46
NETWORK ]
BANGALORE: The Aedes aegypti mosquito that causes chikungunya now seems to
have bitten Bangaloreans. At least 15 persons, suspected to be suffering from the viral
infection, have been admitted to the Epidemic Diseases (ED) Hospital ………. At least
80,000 people in Gulbarga, Tumkur, Bidar, Raichur, Bellary, Chitradurga,
Davanagere, Kolar and Bijapur are affected since December 2005.
Back after 32 yrs, dengue-like fever: chikungunya
Toufiq Rashid
Indian Express.. Thursday, April 27, 2006 at 0000 hrs
Mosquito carrier, not known to be fatal, cases sweep Andhra, Karnataka
NEW DELHI, APRIL 26: Thirty two years after its last outbreak in India, chikungunya is back. A relatively rare viral fever with dengue-like
symptoms, chikungunya has been sweeping Andhra Pradesh, Karnataka and Maharashtra.
In the last three months, the official count of the affected has climbed to a staggering 1.5 lakh people and Health officials concede that
figures on the ground may be higher.
Caused by an alphavirus spread through bites from the Aedes Aegypti mosquito—the same mosquito behind dengue—chikungunya is not
considered fatal. But 77 deaths since 2005 on the Indian Ocean island of Reunion have been linked to chikungunya.
Health officials in Delhi said the last outbreak in the country was reported in 1974. “The
virus must have been silent but it has made a comeback,”
28
Dr.G.C.Sahu/ROH&FW/GoI/Ahmedabad
Dr.G.C.Sahu/ROH&FW/GoI/Ahmedabad](https://image.slidesharecdn.com/chickungunya-dr-120503034555-phpapp02/85/Chickungunya-dr-28-320.jpg)

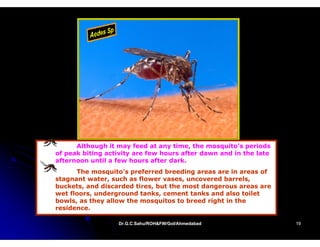
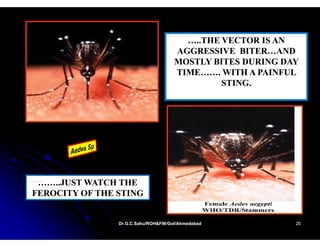
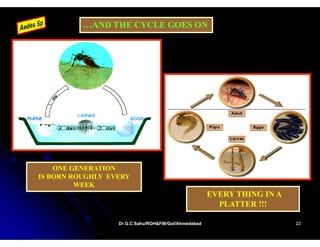
Chikungunya is a viral fever transmitted primarily by the Aedes aegypti mosquito, known for causing debilitating arthritic symptoms and high fever, with outbreaks occurring mainly in Africa, India, and Southeast Asia. The disease, not typically fatal but impairing, has seen significant epidemics in India, particularly since a resurgence around 2005. Prevention focuses on mosquito control and personal protective measures, as there is no specific treatment or vaccine available.










































































