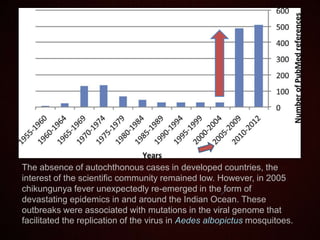
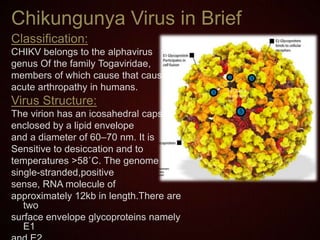
Chikungunya fever, caused by the chikungunya virus (chikv), leads to severe arthritic symptoms primarily transmitted by Aedes mosquitoes. It has seen recent epidemics, notably since 2005, resulting in significant morbidity and long-term health impacts, especially persistent arthralgia. Currently, no licensed vaccine exists, and treatment focuses on symptom relief with ongoing research into antiviral therapies.