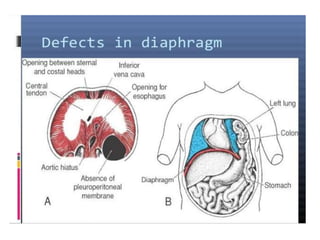
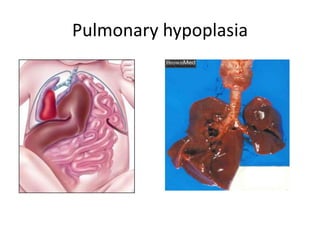
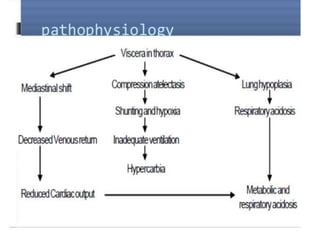
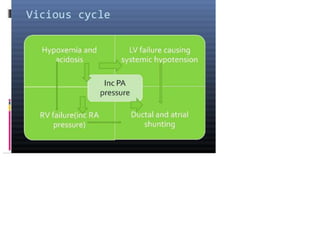
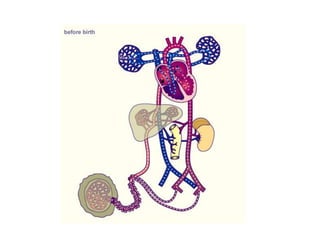
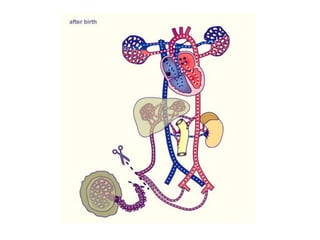
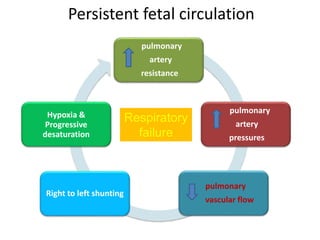
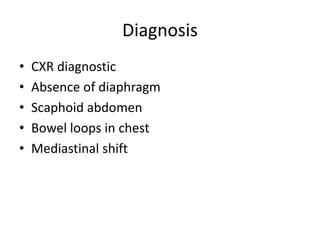
Congenital diaphragmatic hernia (CDH) occurs when abdominal organs protrude into the chest cavity due to a defect in the diaphragm. It has an incidence of about 1 in 2500 births. CDH causes pulmonary hypoplasia and hypertension due to compression of the lungs. Initial treatment focuses on stabilizing the infant medically to improve oxygenation and reverse pulmonary hypertension before repairing the diaphragmatic defect via surgery. Prenatal diagnosis allows for fetal stabilization attempts. Prognosis depends on the degree of pulmonary hypoplasia and hypertension present.














































![CONGENITAL DIAPHRAGMATIC HERNIA [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congenitaldiaphragmaticherniarecovered-240421180720-5c4f960f-thumbnail.jpg?width=640&height=640&fit=bounds)