Superior vena cava (SVC) syndrome is a collection of clinical signs and symptoms resulting from either partial or complete obstruction of blood flow through the SVC.
This obstruction is most commonly a result of thrombus formation or tumor infiltration of the vessel wall.
2. OUTLINE
Introduction
Pathophysiology
Anatomy
Epidemiology
Etiology/Risk factors
Clinical
manifestation
Diagnostic work up
Treatment
Prevention and
control approach
3. Superior vena cava (SVC) syndrome is a
collection of clinical signs and symptoms
resulting from either partial or complete
obstruction of blood flow through the SVC.
This obstruction is most commonly a result of
thrombus formation or tumor infiltration of
the vessel wall.
4. Today, this syndrome is most commonly seen
secondary to malignancy, although there has
been a more recent rise in benign etiologies.
Increased upper body venous pressures
results to venous congestion.
5. Malignant diseases causing SVCO are Lung
cancer (>SCLC and SCC histology cases) which
accounts for nearly 85% of all cases
Followed by Lymphomas mainly NHL 10-15%,
with less than 2% occurs in patients with
Thymomas and mediastinal Germ cell
tumours.
6. Non malignancy causes of SVCO includes
retrosternal goitre, sarcoidosis, tuberculosis,
mediastinal post Irradiation, Idiopathic
fibrosis.
There is also an increase of SVCO in cancer
patents with long term central venous
catheters
7. Mechanisms has divided into three categories
which are compromised vessel anatomy,
impaired venous flow, and diminished vessel
wall integrity (can core exist in PT with SVC
syndrome)
Extrinsic compression and obstruction of the
SVC by a mass in the mediastinum is the most
common cause of SVC syndrome
8. This is often associated with malignancy;
however, there are a variety of nonmalignant
masses.
A growing proportion of SVC syndromes are
now associated with occlusive venous
thrombus formation that compromises venous
flow back to the heart.
9. The increasing use of indwelling intravascular
devices such as catheters and pacemakers
leads have played a major role in this growth.
Resultant venous wall inflammation, fibrosis,
and eventual thrombus lead to stenosis of the
vessel itself
10. The SVC is the major drainage vessel for
venous blood(2cm and a length of
approximately 6-7cm) from the head, neck,
upper extremities, and upper thorax.
It arises from the union of the left and right
brachiocephalic veins, posterior to the first
right costal cartilage.
It descends vertically through the superior
mediastinum, behind the intercostal spaces
and to the right of the aorta and trachea.
At the level of the second costal cartilage,
the SVC enters the middle mediastinum and
becomes surrounded by the fibrous
pericardium.
It terminates by emptying into the superior
aspect of the right atrium at the level of the
third costal cartilage.
It is a thin-walled, low-pressure, vascular
structure. This wall is easily compressed as
it traverses the right side of the
mediastinum.
11. United States statistics
The incidence of SVCS within the United States is
roughly 15,000 cases per year
SVCS develops in 5-10% of patients with a right-side
malignant intrathoracic mass lesion.
In 1969, Salsali and Cliffton observed SVCS in 4.2% of
4960 patients with lung cancer;
In 1987, Armstrong and Perez found SVCS in 1.9% of 952
patients with lymphoma.
12. Age and sex demographics
Malignant causes of SVCS are predominantly
observed in individuals aged 40-60 years.
Benign causes (aged 30-40 years).
SVC in the pediatric age group is rare
Malignant causes of SVCS are most commonly
observed in males ( WHY )
In contrast, cases related to benign causes
show no sex-related differences in
frequency.
13. The most common etiology of SVCS is
malignancy.
Infectious causes ( syphilis, tuberculosis, and
fungus
The most common cause of malignancy-
related SVCS is bronchogenic carcinoma,
which accounts for nearly 80% of cases.
Lymphoma accounts for approximately 15% of
cases.
dialysis catheters and pacemaker are
associated with SVCS. ( WHY )
17. Stridor
Hoarseness
Dysphagia
Pleural effusion
Headache, nausea
Lightheadedness
Syncope
Change in vision,
Altered mental status
Upper body edema
Cyanosis and coma
Horner’s syndrome,
symptoms on one side of
face
Some rare but serious
clinical consequences
reported in SVC syndrome
include
cerebral edema and upper
respiratory compromise
secondary to edema of the
larynx and pharynx.
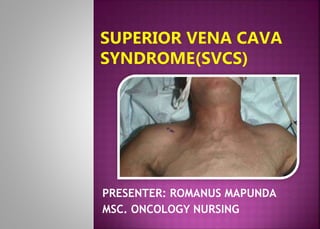
18. The characteristic physical findings of SVCS
include
venous distention of the neck and chest wall,
facial edema, upper-extremity edema, mental
changes, cyanosis, papilledema, stupor, and
even coma.
Bending forward or lying down may aggravate
the symptoms and signs.
19. o Chest X-ray.
o CT and MRI
o Invasive contrast venography.
o Sputum cytology.
o Thoracentesis.
o Bronchoscopy.
o Needle aspiration of a peripheral
lymph node, or mediastinoscopy
20. Elevation of the patient’s head as a simple
maneuver with the goal of decreasing venous
pressure and supplemental oxygen if indicated.
For patients with thrombus related to an
indwelling intravascular device, removal
should be considered along with
anticoagulation (Heparin or Warfarin) therapy
and catheter-directed thrombolysis
21. Emergency treatment is indicated when brain
edema, decreased cardiac output, or upper
airway edema is present
Steroids can be started ( Dexamethasone)
Diuretics
22. Radiation therapy (standard treatment for most
patients with SVCS)
o Dose - 20Gy/ 5 #s or 30Gys/10#s or 37.5Gys/15#s
o The radiation dose depends on tumor size and
radioresponsiveness.
o The radiation portal should include a 2-cm
margin around the tumor.
23. When SVCS is due to thrombus around a central
venous catheter
Patients may be treated with thrombolytics or
anticoagulants (eg, heparin or oral
anticoagulants).
Chemotherapy
o For chemo sensitive tumors.
24. Surgical care:
1. Surgical bypass
May be a useful way to palliate
symptoms(ie, after failure of radiation
therapy and chemotherapy)
2. Stenting
Percutaneous transluminal angioplasty
(PTA), thrombolysis, or some combination
In most patients with SVCS, stenting of the
SVC provides rapid symptomatic relief
within few days
26. Complications of SVCS may include the
following:
Laryngeal edema
Cerebral edema
Decreased cardiac output with hypotension
Pulmonary embolism (when an associated
thrombus is present)
27. Major considerations in the nursing care of
patients with SVCS include
Recognition of high-risk patients
Facilitation and coordination of diagnostic
procedures
Assessment of respiratory, cardiac and neurologic
systems
Administration of therapy
Provision of emotional and psychosocial support, and
Patient education.
28. 1. Azizi AH, Shafi I, Shah N, Rosenfield K, Schainfeld R, Sista A, et
al. Superior Vena Cava Syndrome. JACC Cardiovasc Interv. 2020
Dec 28.
2. Klein-Weigel PF, Elitok S, Ruttloff A, Reinhold S, Nielitz J, Steindl
J, et al. Superior vena cava syndrome. Vasa. 2020 Oct.
3. Flounders JA. Oncology emergency modules: superior vena cava
syndrome. Oncol Nurs Forum. 2003 Jul-Aug.
4. Hassikou H, Bono W, Bahiri R, Abir S, Benomar M, Hassouni NH.
Vascular involvement in Behçet's disease. Two case reports. Joint
Bone Spine. 2002 Jun.
5. Aung EY, Khan M, Williams N, Raja U, Hamady M. Endovascular
Stenting in Superior Vena Cava Syndrome: A Systematic Review and
Meta-analysis. Cardiovasc Intervent Radiol. 2022 Sep.
6. Superior Vena Cava Syndrome (2024)
https://emedicine.medscape.com/article/460865-differential
7. Superior Vena Cava Syndrome (2024)
https://www.ncbi.nlm.nih.gov/books/NBK441981/
Editor's Notes
The superior vena cava is formed by the junction of the left and right innominate (brachiocephalic) veins and is tasked with returning blood from the head, neck, upper extremities, and torso back to the heart.
These are different histological types of lung cancer, each with distinct characteristics and behaviors. Small Cell Lung Cancer is typically more aggressive and tends to spread quickly, while Squamous Cell Carcinoma arises from the squamous cells lining the airways in the lungs and tends to grow more slowly.
Sarcoidosis- autoimmune reaction which make lumps or nodules called granulomas.
These mechanisms often coexist in patients presenting with SVC syndrome
It is located in the middle mediastinum and is surrounded by relatively rigid structures such as the sternum, trachea, right bronchus, aorta, pulmonary artery, and the perihilar and paratracheal lymph nodes. mediastinum. [7]
Malignant causes of SVCS are most commonly observed in males because of the high incidence of lung cancer in this population.
Prior to modern antibiotics, infectious causes including syphilis, tuberculosis, and fungus occurred with almost equal frequency.
Increasingly, dialysis catheters and pacemaker leads are becoming associated with SVCS due to thrombosis.
Typically, symptoms accelerate as the underlying malignancy increases in size and/or invasiveness.
Orthopnea is a medical term used to describe difficulty breathing while lying down flat
Syncope, commonly known as fainting or passing out, is a temporary loss of consciousness due to a sudden decrease in blood flow to the brain
Horner's syndrome is a rare condition caused by damage to a specific set of nerves that control certain muscles and functions of the eye and face
Papilledema is a medical condition characterized by swelling of the optic nerve head (also known as the optic disc)
Invasive contrast venography is the most conclusive diagnostic tool (see the image below). It precisely defines the etiology of obstruction.
A CT scan of the chest is the initial test of choice to determine whether an obstruction is due to external compression or due to thrombosis.
Role of thrombolytic / anticoagulant (Heparin or Warfarin) therapy incases of venous thrombosis