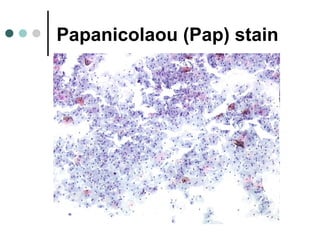
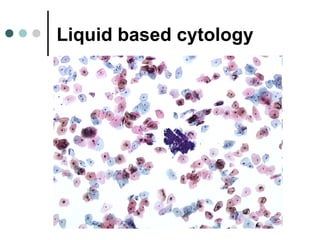


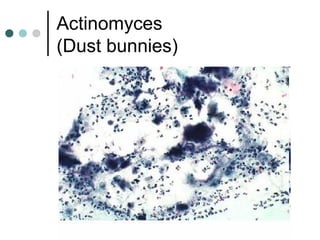
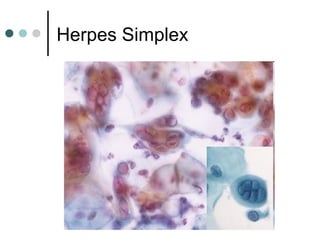
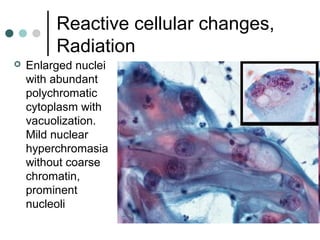
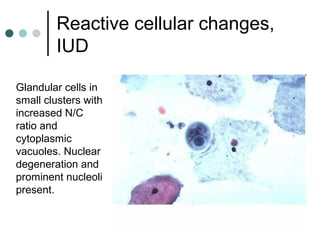
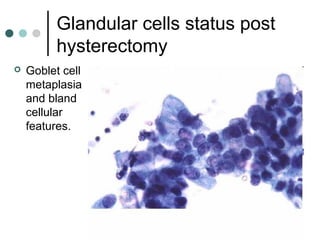
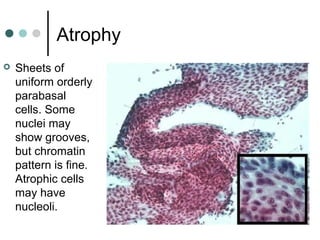
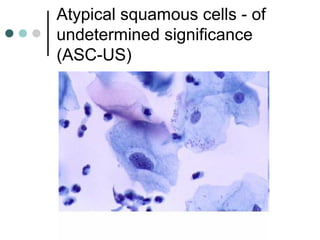
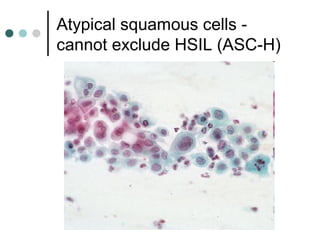
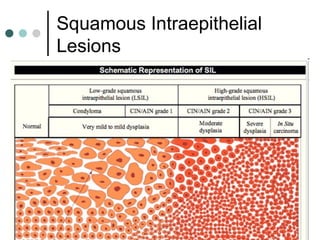



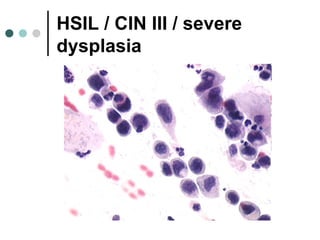
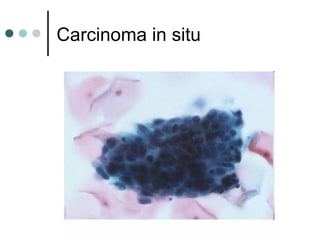
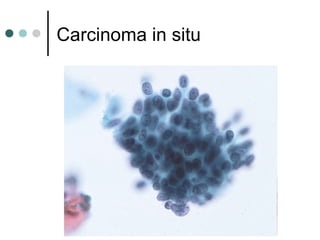
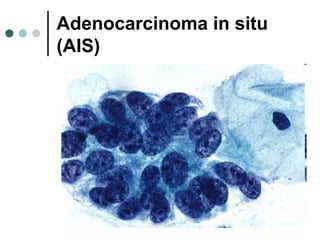
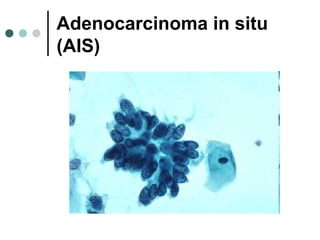
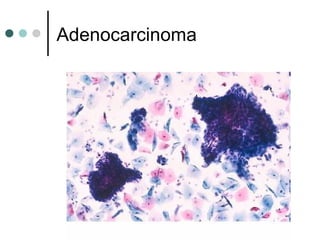



The document provides information on cervical cytology screening and the Bethesda System for reporting results. It describes the Papanicolaou staining technique and liquid-based cytology collection methods. The Bethesda System categories for specimen adequacy, interpretation, and epithelial cell abnormalities are outlined. Normal cervical cell types are defined. Reactive, infectious, and other non-neoplastic findings are described. Atypical squamous cells of undetermined significance, low-grade squamous intraepithelial lesions, and high-grade squamous intraepithelial lesions are defined. Adenocarcinoma in situ and adenocarcinoma are also summarized.































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



